
This post is an answer to the Case – 62-year-old Woman with Nonproductive Cough
Findings
- Chest radiograph shows volume loss on the right with an elevated right hemidiaphragm and right hilum. Right paratracheal opacity is seen in keeping with right upper lobe collapse. The interface with the lung approximates the shape of a reverse S and has come to be known as the (reverse) S sign of Golden. Note the very faint juxtaphrenic peak.
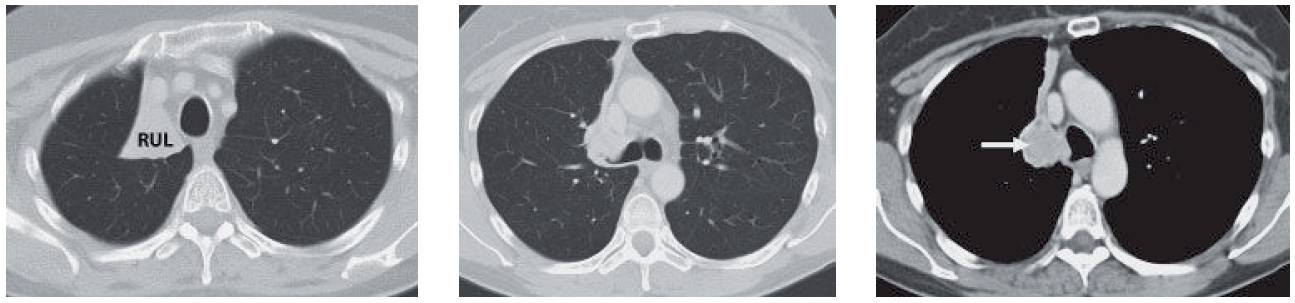
- Follow-up CT confirmed the right upper lobe collapse. This mass obstructs the right upper lobe bronchus and is hyperenhancing. As would be expected, this was a carcinoid tumor.
Differential Diagnosis
Based on the radiograph, the two main concerns would be right upper lobe collapse from a mass or bland right upper lobe collapse.
Teaching Points
- Right upper lobe collapse may be from mucus plugging, peripheral airways disease (such as tuberculosis), or an endobronchial lesion.
- The presence of a central mass creates an inferior bulge that helps create an inverse S between the collapsed lung and the aerated lung.
- Other findings of right upper lobe collapse include a juxtaphrenic peak in which either an inferior accessory fissure or the inferior pulmonary ligament pulls on the hemidiaphragm (akin to marionette strings), an elevated right hilum, and findings of volume loss.
- Rarely, right upper lobe collapse has been associated with a pneumothorax that is thought to result from a vacuum phenomenon. Akin to a joint vacuum phenomenon, this type of pneumothorax has come to be known as a pneumothorax ex vacuo. This pneumothorax will dissipate only if the central mass is cleared. It will not resolve with thoracostomy drainage.
- When right upper lobe collapse is combined with right middle lobe collapse, malignancy should strongly be considered.
Management
With simple collapse, the management rests on pulmonary toilet and occasional bronchoscopy to clear the mucus. The collapse should be compared with prior images or followed to resolution to exclude an underlying mass.
Further Reading
Woodring JH, Reed JC. Radiographic manifestations of lobar atelectasis. J Thorac Imaging. 1996 Spring;11(2):109-44. doi: 10.1097/00005382-199621000-00003. PMID: 8820022.
