This post is an answer to the ECG Case 255
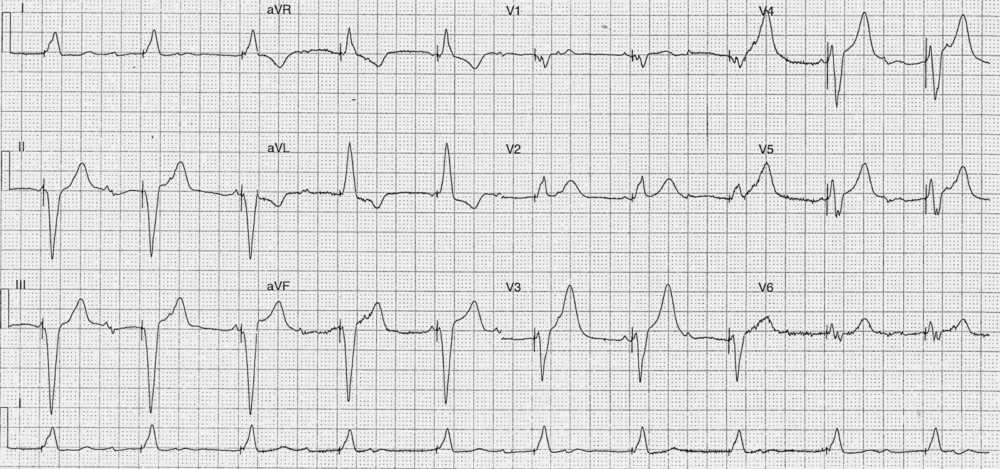
- Rate: 60 bpm
- Rhythm:
- Regular
- Ventricular paced rhythm
- Evidence of non-conducted native atrial activity
- Axis: LAD
- Intervals:
- QRS – Prolonged (160ms)
- QT – 480ms
- Segments:
- Discordant ST / T wave changes in leads I, II, III, aVR, aVL, aVF, V6
- Expected for paced rhythm
- Lead V2
- Concordant ST elevation
- Positive QRS complex with ST elevation <1mm
- NOT an expected change but doesn’t met criteria of =>1mm concordant ST elevation
- Lead V3
- Excessive discordance using Smith’s modified Sgarbossa
- ST elevation ~3mm with QRS depth of 10mm
- ST/T wave ratio of -0.33 (3/-10) which is less than the normal threshold of -0.25
- Lead V4
- Excessive discordance using Smith’s modified Sgarbossa
- ST elevation ~3.5mm with QRS depth of 9.5mm
- ST/T wave ratio of -0.32 (3.5/-11) which is less than the normal threshold of -0.25
- Lead V5
- Baseline wander and P wave superimposition makes ST segment difficult to see
- Potential for excessive discordance
- Disproportionate T wave prominence in leads V2-6
- Discordant ST / T wave changes in leads I, II, III, aVR, aVL, aVF, V6
Interpretation
- V-paced Rhythm
- Modified Sgarbossa Criteria positive given excessive ST discordance in leads V3-5 suggesting possible acute myocardial infarction.
What happened next ?
Given the patients extensive co-morbidities following discussion with cardiology and patient’s family no invasive management was undertaken. The patient had a troponin rise and was treated with optimisation of medical therapy.
This ECG illustrates the challenges and difficulties of interpreting an ECG with LBBB or paced rhythm.