This post is an answer to the ECG Case 258
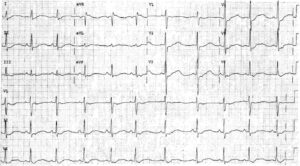
- Rate: 84 bpm
- Rhythm: Sinus arrhythmia
- Axis: Normal
- Intervals:
- PR – Normal (~140ms)
- QRS – Normal (100ms)
- QT – 360ms (QTc Bazette 425 ms)
- Segments:
- ST Elevation in leads II, III, aVF (1-2mm)
- ST Depression in leads I, aVL, V1-3
- Additional:
- Dominant R waves lead V1-3
- Prominent T waves leads V2-3
Interpretation
Inferior ST elevation with posterior involvement
What happened next ?
The patient was taken for urgent angio which showed a isolated spontaneous dissection of OM1. The lesion was not stented and the patient was treated with medical therapy and anti-coagulation.
Subsequent echo showed normal valves and right ventricular functions with left ventricular mild-moderate infero-lateral-apical akinesia with an EF of 52%. The patients initial troponin T was 37.4 ug/L.
Spontaneous Coronary Artery Dissection
- This is a very rare phenomenon found at ~0.1% of all angios
- Affects young people with a mean age of 35-40 years
- Major predominance for females accounting for 70% of cases
- Etiology not fully understood
- Associations with peripartum, trauma, and connective tissue diseases
- Can occur in the setting of atherosclerotic disease and no cause may be found
- Higher risk of complications with PCI so the majority are treated with medical management