This post is an answer to the ECG Case 326
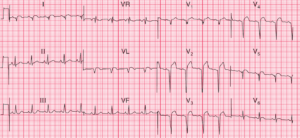
- Rate:
- Ventricular rate ~36 bpm
- Atrial rate ~72 bpm
- Rhythm:
- Regular ventricular complexes
- Regular atrial complexes
- 2:1 AV Block
- Axis: Right axis deviation
- Intervals:
- PR – Normal (~160-180ms)
- In conducted complexes
- QRS – Prolonged (120ms)
- PR – Normal (~160-180ms)
- Additional:
- RBBB Morphology
- Not entirely classic appearance
- ST Depression in leads II, III, aVF, V2-4
- ST Elevation in lead aVL
- Only 1 full complex captured which has 1mm STE
- Partially captured ST segment shows less ST elevation
- ? Artefact
- Biphasic T wave in leads V2-3
- RBBB Morphology
Interpretation
- 2:1 AV block
- QRS Prolongation favours Mobitz II / Infra-nodal block
- Abnormal QRS morphology and ST/T wave changes
The ST and T wave changes on the ECG are interesting and raise the question of potential causes for the conduction abnormality. Differentials for these features include:
- Ischaemia / ACS
- Electrolyte Abnormality
- Drug effect especially digoxin
- Cardiomyopathy
- Myocarditis
- Hypothermia
- Hypothyroid / Hyperthyroid
Interestingly in our case there was no discernible or reversible cause identified for her conduction abnormality.
What happened next ?
The patient was commenced on i.v. isoprenaline infusion due to symtomatic nature of the bradyarrhythmia. Medication review found no culprit medication and her electrolytes and cardiac biomarkers were normal. She underwent an uncomplicated dual chamber PPM insertion, settings DDD-CLS 60-130 bpm, and was discharged following a brief in-patient stay. The DDD code refers to pacing and sensing of both atria and ventricles with potential response of either inhibition or triggering of pacing.
READ MORE: Conduction Blocks at the AV Node (AV Blocks) [With Examples]