
This post is an answer to the Case – 69-year-old Woman with Hemoptysis
Findings
- On the initial radiograph, the right heart border and hemidiaphragm are obscured.
- Associated volume loss is noted, which can best be seen by the rightward shift of the heart and mediastinum.
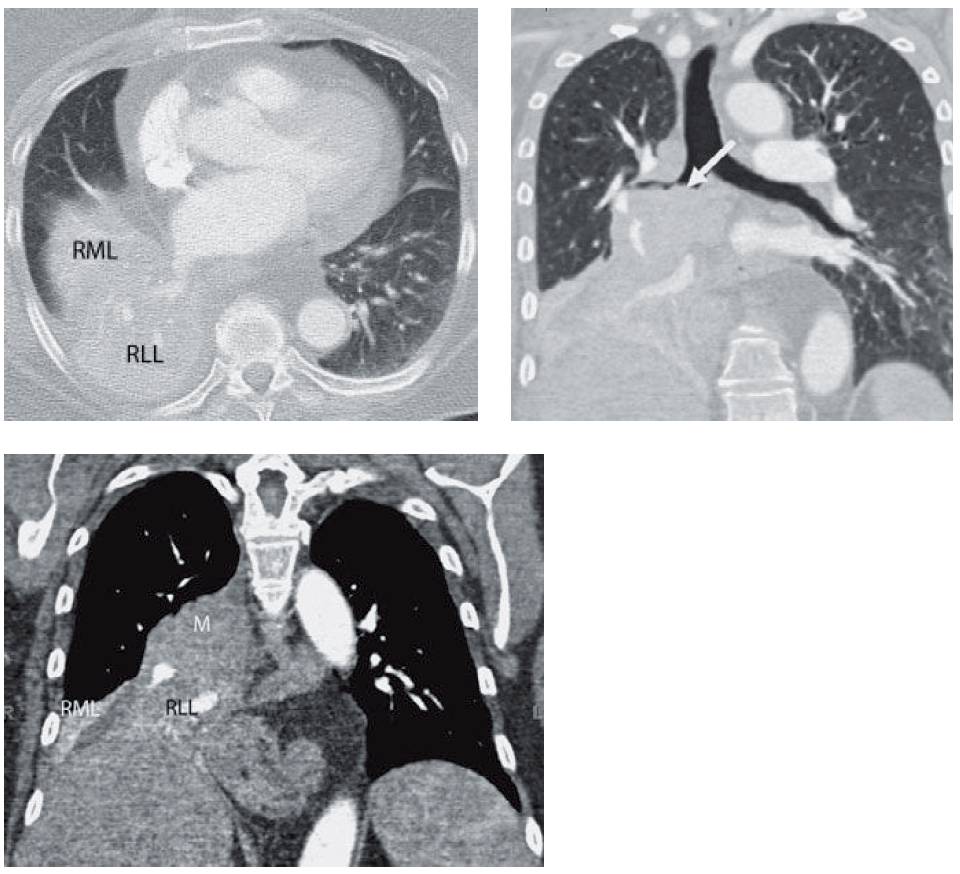
- CT was performed the next day, which showed the collapsed lobes (RML = middle lobe and RLL = right lower lobe). Reconstructions more clearly delineate the central mass (white arrow) and the collapsed lobes (RML = middle lobe, RLL = lower lobe, and m = mass).
Differential Diagnosis
Based on the radiograph, right middle lobe and right lower lobe collapse should be the main consideration.
Teaching Points
- Right middle and lower lobe collapse is the result of obstruction of the bronchus intermedius, from either mucus or an endobronchial lesion.
- The volume loss of both lobes results in inferior displacement of the minor and major fissures. Usually, the minor fissure falls below the level of the major fissure and the major fissure extends superiorly to the hilum. The net composite is the “S-shaped” opacity as seen above, especially when a central mass is present.
- Right middle and lower lobe collapse displaces the right hilum inferiorly and obscures the descending right interlobar artery.
- Shift of the heart and mediastinum rightward is frequently seen with this combination of collapse.
- To prevent confusion with a right pleural effusion, one must remember that an effusion is higher laterally and combined right middle and lower lobe collapse is higher medially.
- The double lesion sign refers to collapse of two segments that are not in proximity. Because of the anatomic distance, a single lesion (cancer) is not plausible. An example of the double lesion sign would include right upper and lower lobe collapse without middle lobe involvement.
Management
With simple collapse, the management rests on pulmonary toilet and occasional bronchoscopy to clear the mucus. Collapse should be compared to a prior study or followed to resolution to exclude a central mass.
Further Reading
Woodring JH, Reed JC. Radiographic manifestations of lobar atelectasis. J Thorac Imaging. 1996 Spring;11(2):109-44. doi: 10.1097/00005382-199621000-00003. PMID: 8820022.
