A 66-year-old man presented to the emergency department with a 3-day history of cough, congestion, and pain in his chest and the left side of his abdomen. Several months before presentation, he had immigrated to the United States after living in a refugee camp for 20 years.
The results of the physical examination were notable for heart sounds best heard on the right side of the chest and for tenderness in the costochondral joints and the left upper quadrant on palpation.
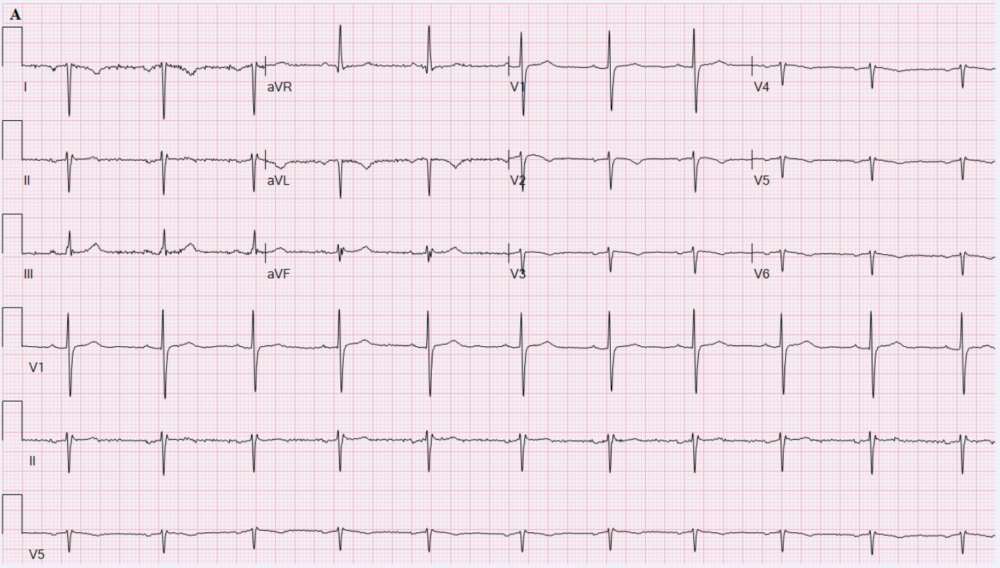
An electrocardiogram showed right axis deviation, reverse precordial R-wave progression, and inverted P waves in leads I, aVL, and aVR .
Findings on a chest radiograph included dextrocardia (Panel A), and computed tomography of the abdomen revealed mirror-image transposition of the abdominal organs (Panel B), confirming the presence of situs inversus totalis without acute pathologic features.
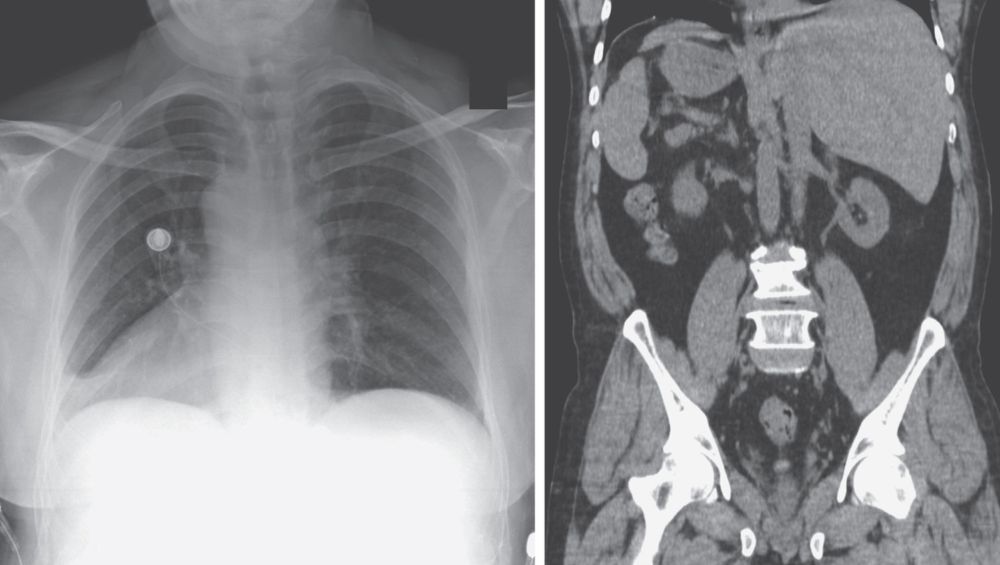
Situs inversus totalis can occur in isolation or in conjunction with primary ciliary dyskinesia. The patient had no history of recurrent respiratory infections suggestive of primary ciliary dyskinesia. Echocardiography revealed no structural abnormalities.
A diagnosis of upper respiratory infection was made, and the musculoskeletal chest pain was treated with nonsteroidal antiinflammatory drugs. The infection resolved several days after presentation.