This post is an answer to the ECG Case 247
- Rate: 66 bpm
- Rhythm:Regular Sinus rhythm
- Axis: RAD
- Intervals:
- PR – Normal (120ms)
- QRS – Normal (80ms)
- QT – 400ms (QTc Bazette 420 ms)
- Segments: Normal
- Additional:
- T wave inversion in leads I, aVL, V1
- Negative P waves in lead I, aVL
- Notched P wave in inferior leads
- Q waves infero-lateral leads (leads II, III, aVF, V4-6)
- Narrow Q waves
- Depth ~2 mm but maximal in V5 at 3mm. All <25% of QRS voltage
- Early R wave transition
Interpretation
- RA-LA lead reversal
- Infero-lateral Q waves
- Normal variant vs structural disease
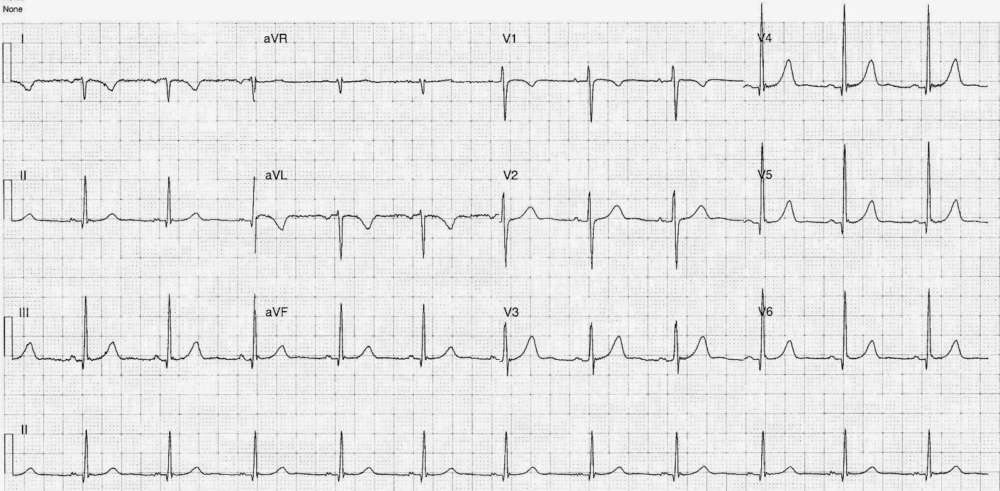
The presence of complete inversion (P-QRS-T) of any lead, expect aVR, should alert to potential lead reversal as should an ECG with abnormal axis. RA-LA is probably the most commonly encountered lead misplacement and results in:
- Inversion of lead I
- With resultant RAD, assuming native axis is normal
- Leads II and III switch places
- Leads aVR and aVL switch places