This article is an answer to the ECG Case 48
ECG Interpretation
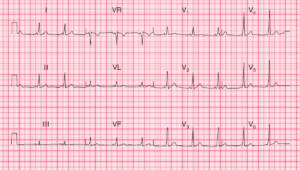
- Sinus rhythm, rate 65/min
- Peaked P waves, best seen in lead II (P pulmonale)
- Right axis deviation (RAD)
- Dominant R waves in lead V1
- Deep S waves in lead V6
- Inverted T waves in leads II, III, VF, V1–V3 (right ventricular strain pattern)

Clinical Interpretation
This combination of right axis deviation, dominant R waves in lead V1 and inverted T waves spreading from the right side of the heart is classic of severe right ventricular hypertrophy.
Right ventricular hypertrophy can result from congenital heart disease, or from pulmonary hypertension which may be idiopathic, secondary to mitral valve disease, lung disease, or pulmonary embolism.
The physical signs of right ventricular hypertrophy are a left parasternal heave and a displaced but diffuse apex beat. There may be a loud pulmonary second sound. The jugular venous pressure may be elevated, and a ‘flicking A’ wave in the jugular venous pulse is characteristic of pulmonary hypertension.
What to do next?
The two main causes of pulmonary hypertension of this degree in a 40-year-old woman are recurrent pulmonary emboli, and idiopathic (primary) pulmonary hypertension.
Clinically, it is difficult to differentiate between the two, but a lung scan and CT pulmonary angiography will help. In either case, anticoagulants are indicated.
In fact, this patient had primary pulmonary hypertension and treatment with high dose calcium channel blockers, prostanoids, endothelin receptor antagonists (bosentan) and phosphodiesterase inhibitors was tried, without success. Eventually she needed heart and lung transplantation.