This post is an answer to the ECG Case 301
- Rate: 84 bpm
- Rhythm: regular sinus rhythm
- Axis: Normal
- Intervals:
- PR – Normal (~160ms)
- QRS – Normal (90ms)
- QT – 400ms (QTc Bazette 435 ms)
- Segments:
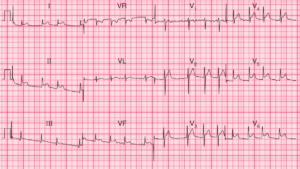
- ST elevation in lead aVL (<1mm) and lead I (2nd and 3rd complexes <1mm)
- ST depression in leads II, III, aVF
- Additional:
- Up-sloping ST segment V6
- T wave inversion in leads III, aVR, V1
- Interpretation:
- High lateral changes suspicious for ACS
What happened next ?
Following discussion with the cardiology team the patient was transferred for primary angioplasty given on-going chest pain and progressive ECG features.
Coronary angiogram showed:
- LM – Normal
- Cx – Dominant with irregularities
- LAD and RCA – irregularities
- LV gram – Apical Hypokinesis
Subsequent echo showed:
- Normal LV size and thickness.
- Hypokinesis of mid to apical anterolateral, anterior and inferior lateral regions with normal systolic function.
Given echo and angiogram findings the patient was diagnosed with Takotsubo cardiomyopathy. She was commenced on beta-blocker therapy and discharge with out-patient follow-up.