
ECG Interpretation
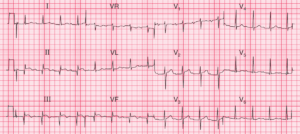
- Sinus rhythm, rate of sinus beats 75/min
- Second degree Type I (Wenckebach) AV heart block (most obvious in the rhythm strip, recorded from lead II)
- Ventricular rate 70/min
- Normal axis
- Small Q waves in leads II, III, VF
- ST segment elevation in leads II, III, VF and reciprocal ST depression in leads I, aVL (inferior stemi)
- ST segment depression in leads V2–V6, maximal in leads V2-4 (posterior stemi)

Clinical Interpretation
This patient has second degree type I AV block of the Wenckebach type (progressive lengthening of the PR interval followed by a nonconducted P wave, and then a return to a short PR interval and repeat of the sequence).
There is also clear evidence of acute inferior and posterior ST segment elevation myocardial infarction (STEMI). The involvement of the posterior wall is indicated by the ST depression maximal in leads V2-V4.
What to do ?
The patient should be treated in the usual way for his acute myocardial infarction, with pain relief and immediate percutaneous coronary intervention (PCI) or thrombolysis.
Wenckebach second degree type I AV block is usually benign when it occurs with an inferior infarction, and although he must obviously be monitored until sinus rhythm with normal conduction returns, temporary pacing is not necessary.
- READ ALSO:
- More Similar Cases:
![Read more about the article Conduction Blocks at the AV Node (AV Blocks) [With Examples]](https://manualofmedicine.com/wp-content/uploads/2021/05/Excerpt-AV-Blocks-300x243.jpg)
![Read more about the article Hypokalemia ECG Changes [With Examples]](https://manualofmedicine.com/wp-content/uploads/2021/04/Hyperkalemia-and-Hypokalemia-ECG-Changes-2-300x127.jpg)