This post is an answer to the ECG Case 315
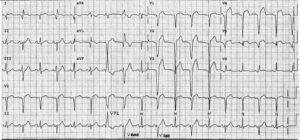
- Rate: 72 bpm
- Rhythm: Regular sinus rhythm
- Axis: Normal
- Intervals:
- PR – Short (~100ms)
- QRS – Prolonged (110-120ms)
- Segments:
- ST Elevation in leads II, III, aVF, V5-6
- ST Depression in lead aVL
- Additional:
- Delta wave
- Biphasic T wave in V2-4
- T Inversion in lead aVL
Interpretation
- Wolff-Parkinson-White / Pre-excitation
- Short pr
- Delta wave
- QRS Prolongation
- Type ‘A’ Pattern / Left sided accessory pathway
- Left posterior AP using Modified Arruda Algorthm
- ST changes on single ECG could be secondary to pre-excitation vs ACS
What happened next ?
This patient had no old ECG’s for comparison and had never been given a diagnosis of pre-excitation before today. The nature and history of the chest pain was suspicious of myocardial ischaemia. The patient was pain-free following initial ED treatment and serial ECG’s did not show dynamic changes. He had raised troponins, peak trop I 0.28 ug/L, and underwent angiography which showed:
- LM: Normal
- LAD: Mild – mod / mild disease
- Cx: Normal
- RCA: 70% mid stenosis – PCI with BMS
Post stent echo showed:
- Normal LV size and function
- Basal posterior wall motion abnormality due to pre-excitation
- Normal RV size and function
The patient was commenced on DAPT, statin and beta-blocker therapy with planned electro-physiologist follow-up for EPS +/- ablation.
This case highlights the challenges of assessing for acute ischaemia in the setting of pre-excitation in this scenario clinical suspicion, serial ECG’s and comparison with old ECG’s are paramount. This are no ‘rules’ we can apply in these scenarios to differentiate acute ischaemia from the abnormalities seen due to pre-excitation.
READ MORE: ECG Interpretation – All you need to know