This post is an answer to the ECG Case 329
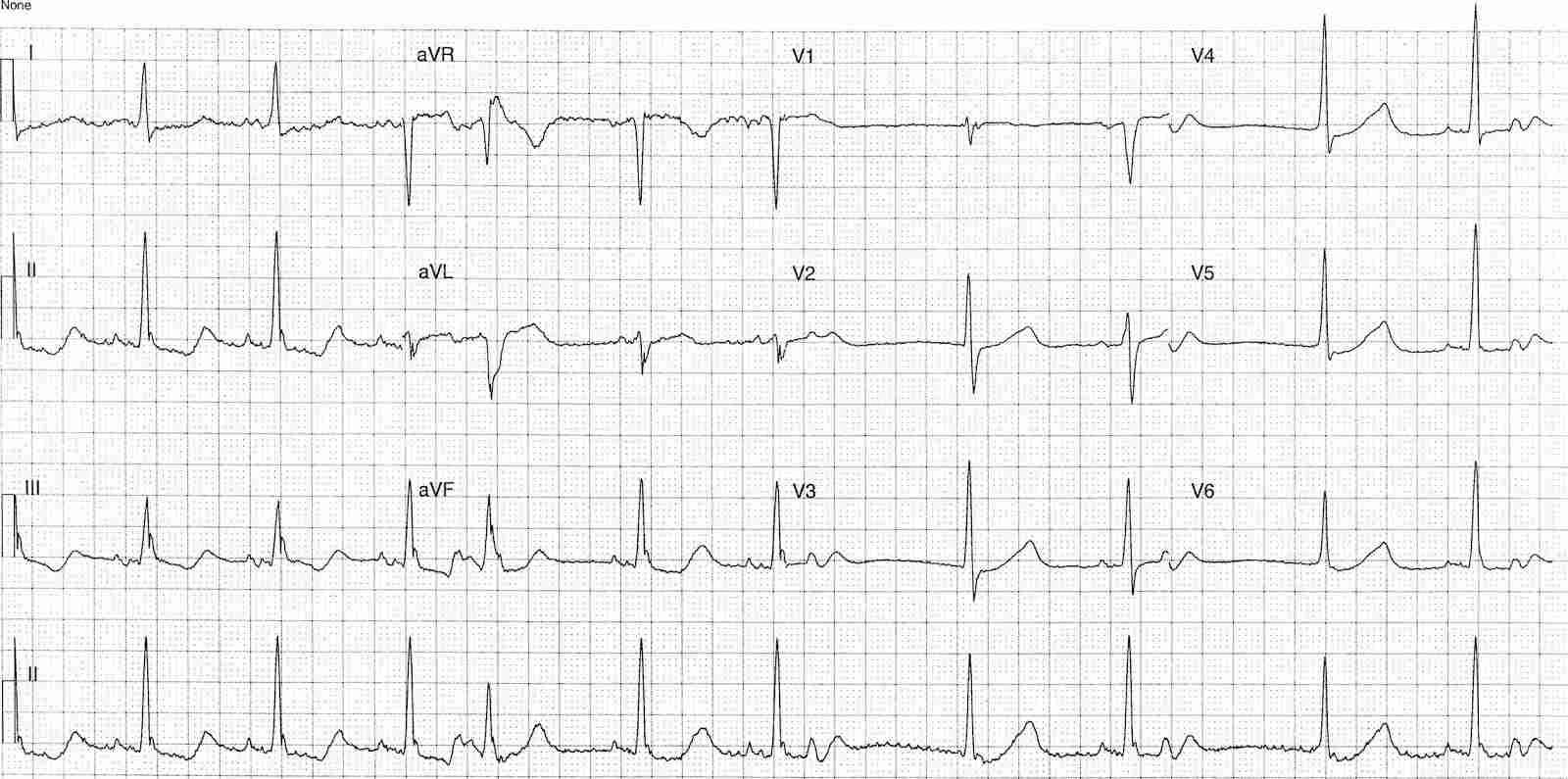
- Rate: Mean rate 66 bpm
- Rhythm:
- Irregular
- Complexes #1-3, 5-6, 8-10
- Sinus rhythm
- Complex #4
- PVC
- Complexes #7 & 9
- No convincing preceding P wave
- Similar morphology as sinus complexes
- Potential junctional escape during period of sinus arrest / pause
- Axis: Normal
- Intervals:
- PR – Normal
- During sinus conduction
- QRS – Prolonged (120ms)
- QT – 520ms (QTc Bazette 565 ms)
- Calculated in lead II using consecutive sinus complexes
- PR – Normal
- Additional:
- Absence of typical BBB pattern
- ST Depression in leads II, III, aVF, V3-6
- Biphasic (down-up) T wave in inferior leads
- Baseline artifact
- Notching in ST segment in complexes #6,8,10
- Precedes period of sinus pause and junctional escape
- ? Increased sinus automaticity during ventricular refractory period
Interpretation
- QT Prolongation
- ST Depression
- Increased automaticity
- PVC, Rhythm disturbance, PJC, possible increased sinus acitivty
Favors hypokalemia and/or hypomagnesemia as the likely cause.
What happened next ?
The patient’s biochemistry results were:
- Na 131 mmol/L
- K 2.2 mmol/L
- Cl 73 mmol/L
- Bicarb 44 mmol/L
- Urea 20.3 mmol/L
- Creat 153 umol/L
Both calcium and magnesium were within normal limits. The patient was on a combination angiotensin II receptor antagonist and thiazide diuretic which was ceased and following electrolyte correction her confusion resolved.
READ MORE: Hypokalemia ECG Changes [With Examples]
SIMILAR CASES: