This post is an answer to the ECG Case 332
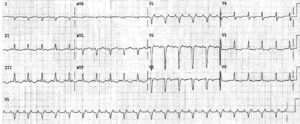
- Rate: 48 bpm
- Rhythm:
- Irregular
- No P waves visible
- Axis: Right axis deviation
- Intervals: QRS – Prolonged
- Additional:
- ST Elevation in leads I, aVL, V1-4
- ST depression in leads III, aVF
- Bizarre broad QRS without typical BBB
- Prominent T waves in leads V3-6
- Key abnormalities:
- Slow atrial fibrillation
- QRS Prolongation
- High lateral ST elevation
- Prominent precordial T waves
The differentials of these ECG findings are relatively broad but the immediate life-threats would be:
- Acute myocardial infarction
- Hyperkalaemia
- Drug toxicity
Other causes include myocarditis, cardiomyopathy and hypothermia.
We must always take our ECG differentials to the bedside and consider them within the clinical presentation and scenario. ECG abnormalities in the acutely unwell diabetic should always prompt consideration of hyperkalaemia and acid-base disturbance as the primary cause.
We must also be mindful that diabetic emergencies can be precipitated by acute cardiac ischaemia and also cause hypercoagulable states. This patient had no associated chest pain nor any history of cardiac disease.
The patients initial VBG showed diabetic ketoacidosis (DKA) with severe hyperkalemia of 8.7 mmol/L.
READ ALSO:
SIMILAR CASES: