ECG Intepretation
The rhythm is primarily regular at a rate of 60 bpm. There are P waves (*) before each QRS complex with a stable PR interval (0.16 sec).
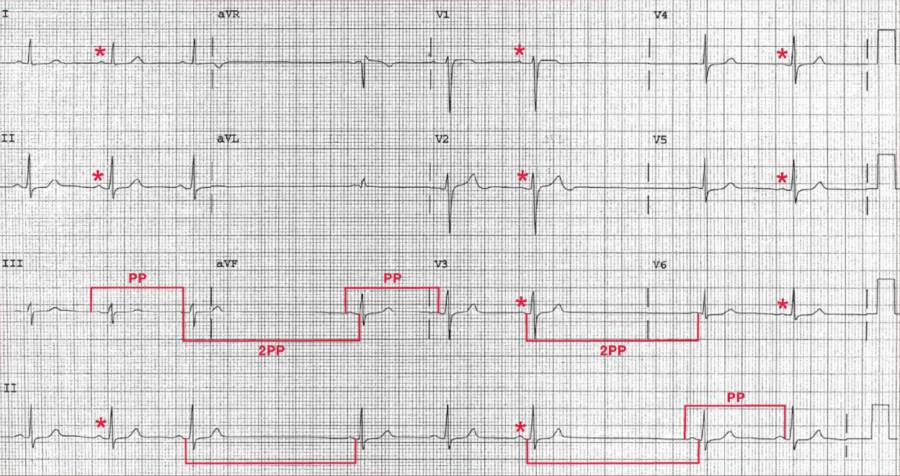
There are two long RR (or PP) intervals without any P wave during the intervals (U). These represent two sinus pauses, the duration of which is equal to two sinus intervals (n) (based on measurement of the PP intervals of the two sinus complexes immediately before and after the pauses). Therefore, this represents sinus node exit block.
The QRS complex duration (0.08 sec) and morphology are normal. The axis is normal, between 0° and +90° (positive QRS complex in leads I and aVF). The QT/QTc intervals are normal (400/400 msec).
Sinus Node Exit Block
With sinus node exit block, the sinus impulses are regular but there is a failure of one sinus impulse to exit the sinus node area to activate the atria; hence no P wave is present. Since the sinus node impulses are regular, the PP interval around the pauses is equal to two sinus intervals.
The slowing of the sinus rate due to sinus node exit block with light pressure on the carotid artery is a manifestation of carotid sinus hypersensitivity (CSH). CSH is an exaggerated carotid baroreceptor response that results in dizziness or syncope from bradycardia (cardio-inhibitory response) or peripheral vasodilation (vasodepressor response).
Bradycardia can be due to sinus node and/or AV node dysfunction. Increased transmural pressure of the carotid sinus creates afferent impulses to the nuclei tractus solitarius in the brain stem, resulting in efferent impulses via the sympathetic and vagus nerves that affect heart rate and vasomotor tone.
Carotid Sinus Hypersensitivity (CSH)
CSH is typically seen in elderly patients and is associated with underlying neck pathology such as tumors, post-surgical scarring, or radiation fibrosis. The reproduction of symptoms and bradycardia with carotid sinus massage confirms the diagnosis of CSH.
Management
Management includes stopping all nodal suppressive agents and maintaining adequate intravascular volume. Persistence of these symptoms in a patient with syncope due to cardio-inhibitory CSH is a class I indication for permanent pacemaker placement.
SIMILAR CASE: ECG Case 93: Sick Sinus Syndrome