ECG Interpretation
The rhythm is irregular, but there is a pattern to the irregularity; that is, all the long intervals are the same, the short intervals are the same, and the intermediate intervals are the same. Hence the rhythm is regularly irregular.
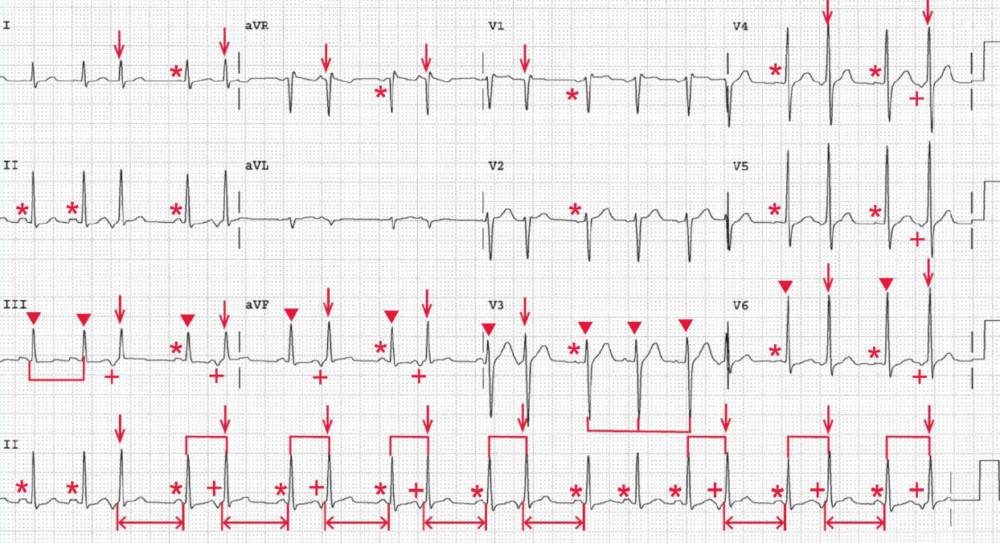
There is an underlying regular rhythm at a rate of 118 bpm (ie, the intermediate intervals). There is a P wave (*) before each of the regular QRS complexes (▼) as well as before the QRS complexes that follow the long RR intervals and are associated with the intermediate RR intervals, and the P wave is positive in leads I, II, aVF, and V5-V6; hence this is sinus tachycardia.
The QRS complex duration (0.08 sec) and morphology are normal. The axis is normal, between 0° and +90° (positive QRS complex in leads I and aVF). The QT/QTc intervals are normal (320/450 msec).
There are occasional QRS complexes that are early or premature, and before each of these complexes is a P wave (+) that is different than the P waves that originate in the sinus node (ie, the P wave is negative in leads II, aVF, and V4-V6).
The QRS complex duration, morphology, and axis are identical to those of the sinus QRS complexes. Therefore, these are premature atrial complexes (PACs). Since each PAC has the same abnormal P-wave morphology, these are unifocal PACs.
After the PAC there is a pause (<->) (ie, long RR interval), the duration of which is variable. That is, the PP interval surrounding the pause may be shorter than, longer than, or equal to two sinus (PP) intervals.
In this case, the PP interval surrounding the pause is equal to two PP intervals. Hence this is called a full compensatory pause.
The pause after the PAC is due to the fact that the premature atrial impulse can affect the sinus node, suppressing or resetting its activity. Hence the duration of time before the occurrence of the next sinus impulse is variable. In this case the PAC has suppressed the sinus node, which thereafter generates an on-time P wave.
What are PACs (Premature Atrial Complexes)
The most common mechanism of PACs is enhanced automaticity of a specific atrial focus; however, a reentrant circuit within the atria can also cause PACs.
PACs occur in individuals of all age groups and can occur in the presence or absence of heart disease. However, the frequency of PACs is higher in patients with structural heart disease, particularly those with left atrial enlargement or hypertrophy, as in the case of mitral valve disease or left ventricular dysfunction. PACs may serve as triggers for other atrial arrhythmias such as atrial fibrillation.
PACs are common, benign, and often asymptomatic, although they can be associated with palpitations or the sensation of skipped beats. No treatment is indicated for the patient who is asymptomatic.
However, for symptomatic individuals, the first step in treatment is to avoid precipitating causes such as caffeine, alcohol, smoking, and stress.
If this initial approach is unsuccessful, then a beta-blocker can be initiated for treatment of symptoms associated with PACs. A beta-blocker does not usually suppress PACs but may reduce symptoms, which are often the result of post-extrasystolic potentiation resulting from the PAC and pause.