This post is an answer to the ECG Case 219
- Rate:
- Mean ventricular rate 42 bpm
- Atrial rate 78 bpm
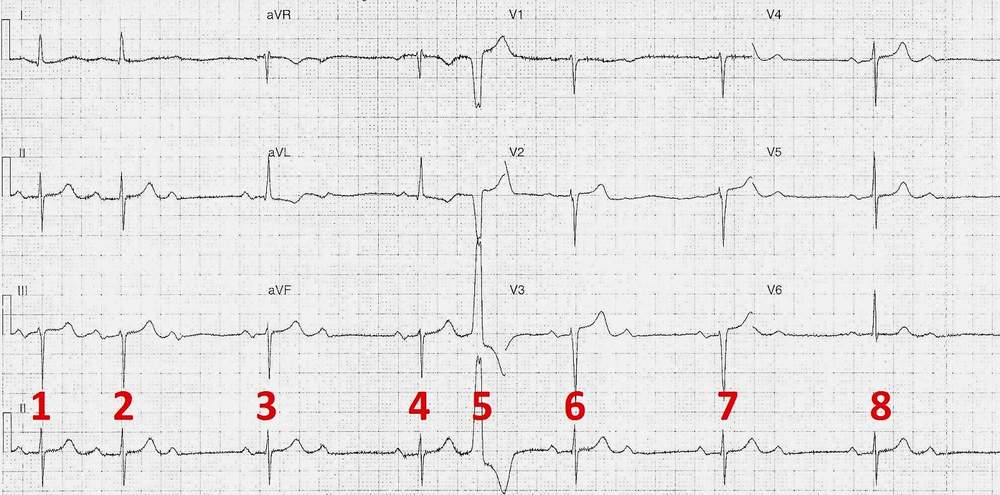
- Rhythm:
- Complexes # 1, 2, 3, 4, 6, 7, 8
- Preceded by P wave
- Progressive PR lengthening from complexes 1 & 2
- 240ms to 280ms
- Non-conducted atrial complexes between complexes # 2 & 3, 3 & 4, 6 & 7
- PVC
- Complex #5
- Complexes # 1, 2, 3, 4, 6, 7, 8
- Axis: LAD
- Intervals:
- PR – Prolonged (~240ms)
- Complexes #1, 3, 4, 6, 7 , 8
- Complex # 2 PR ~280ms
- QRS – Normal (100ms)
- QT – 400ms
- PR – Prolonged (~240ms)
- Segments:
- ST Elevation leads III, aVF, V2-4 (all <1mm)
- Nil ST depression
- Additional:
- Late R wave transition
- Near voltage criteria for LVH
Interpretation
- Initial 2nd Degree AV Block Type 1 (Mobitz I)
- 2:1 AV Block
- Single PVC
What happened next ?
The patient was asymptomatic at rest in the Emergency Department and symptoms had been variable over the preceding weeks. The patient was admitted under the cardiology team and during her in-patient stay remained relatively asymptomatic despite multiple cardiac rhythm changes, including Mobitz I, Mobitz II, and Complete Heart Block, with ventricular rates as low as 30 bpm being well tolerated.
Echo showed:
- Mild / Moderate Aortic Stenosis
- Moderate Pulmonary Hypertension
- Mitral Stenosis with Moderate Mitral Regurgitation
- Severe Left Atrial Dilation
- Normal LV function
Following discussion with the patient and given her functional status a PPM was inserted.
READ MORE:
SIMILAR CASES: