Table of Contents
Atrioventricular block (AVB) is a broad term that encompasses several dysrhythmias that range in severity from benign to life threatening.
First degree AVB is the most common type of AVB and is characterized by a prolonged P-R interval. In the majority of patients with first-degree AVB, no treatment is necessary.
In contrast to first-degree AVB, third-degree AVB is characterized by complete atrioventricular (AV) dissociation and requires immediate treatment to prevent cardiovascular collapse.
Second-degree AVB is divided into two types, Mobitz type I and type II. It is important for the emergency provider to be able to distinguish between these two types of second-degree AVB, as treatment, disposition, and prognosis can be vastly different.
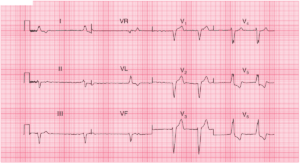
Mobitz type I AV Block (Wenckebach)
Mobitz type I AV Block, also known as Wenckebach, is generally seen in younger patients and athletes. Though it is considered a benign dysrhythmia, it can occasionally present in older patients and be an early warning of more advanced disease of the conduction system.
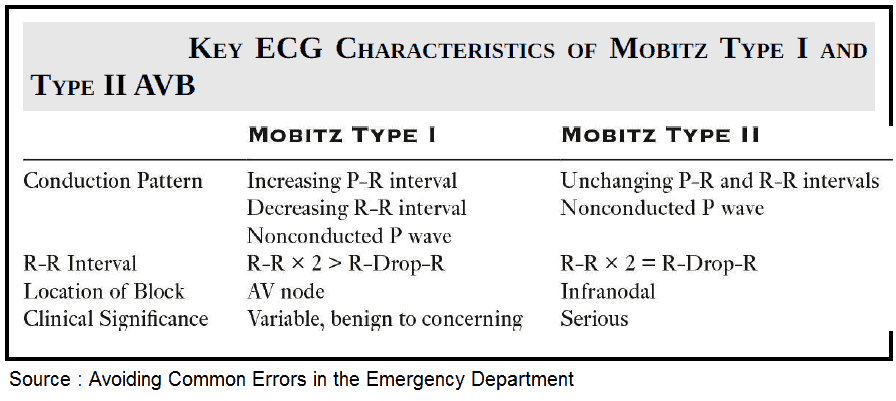
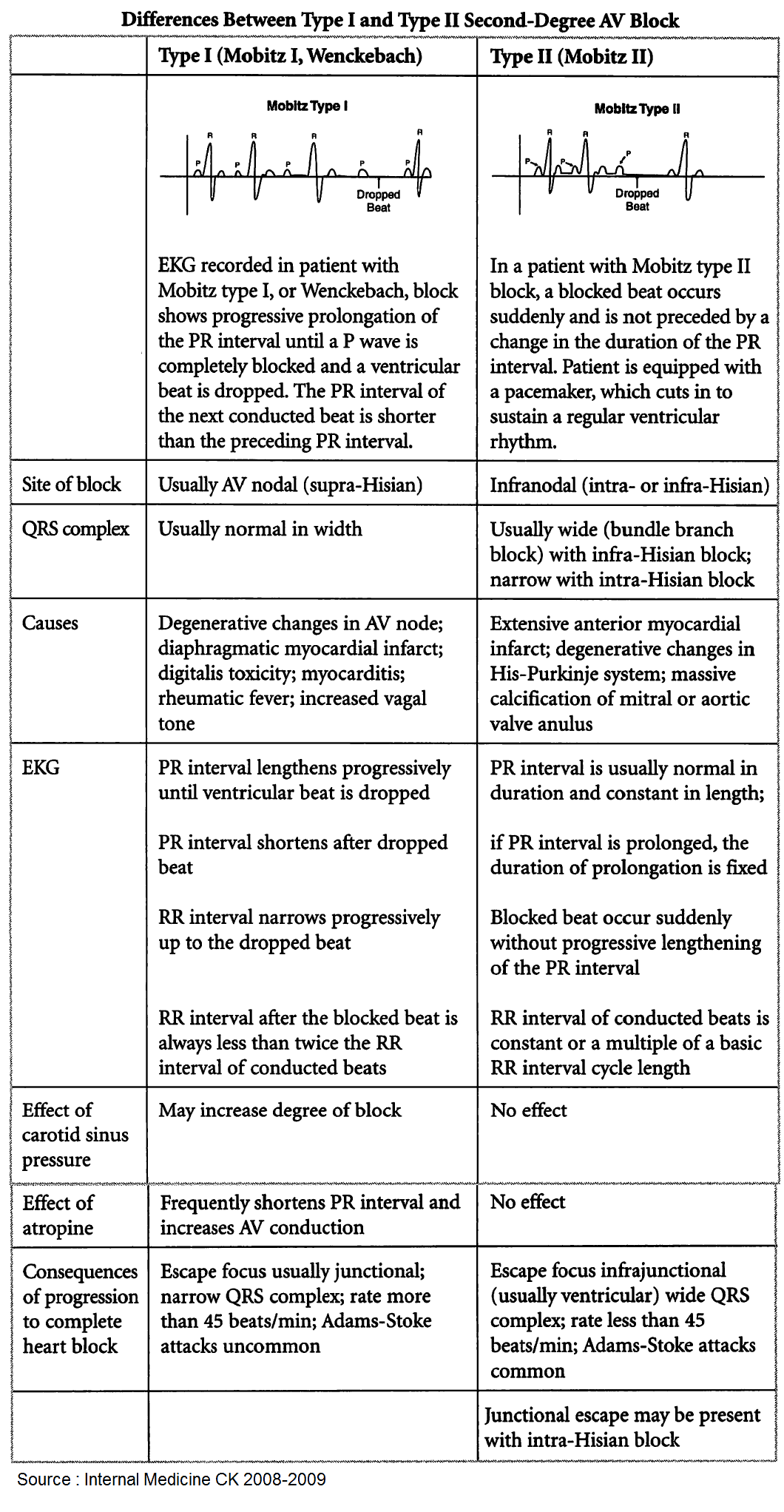
The electrocardiogram (ECG) characteristics of Mobitz type I AVB include the progressive lengthening of the P-R interval and the progressive shortening of the R-R interval, followed by a nonconducted P wave. This produces a characteristic and distinctive pattern of grouped beats on the ECG.
The most common location of conduction block in Mobitz type I is at the level of the AV node. Essentially, there is a gradual increase in conduction delay at the AV node, which eventually results in a nonconducted P wave and a dropped ventricular beat.
Most patients with Mobitz type I AVB are asymptomatic and require no additional evaluation or treatment. This rhythm rarely, if ever, results in hemodynamic compromise or progresses to third-degree AVB.
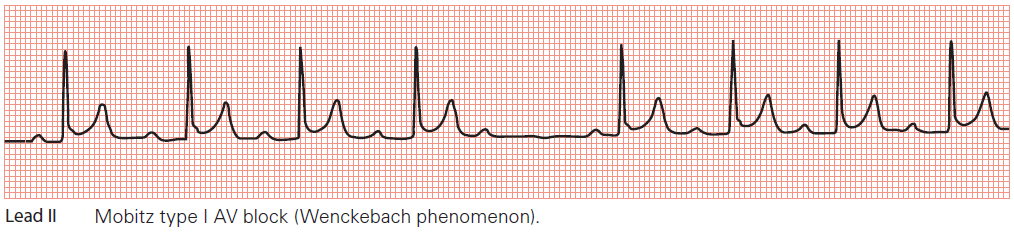
Key points: • The PR interval gradually lengthens until a P wave fails to be conducted.
• The PR interval resets, and the cycle repeats.
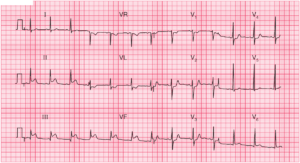
Mobitz type II AV Block
Mobitz type II AV Block is always abnormal, usually associated with significant heart disease, and has a high rate of progression to complete heart block (CHB). Mobitz type II AVB should never be considered a benign ECG finding.
In contrast to Mobitz type I AVB where the conduction block is at the level of the AV node, the conduction delay of Mobitz type II is usually below the AV node.
The characteristic ECG findings in type II AV Block include a constant P-R interval with sporadic and unpredictable nonconducted P waves. Unlike type I AVB, there is no distinguishable ECG pattern in type II AV Block.
As mentioned, patients with type II AV Block are at greater risk of symptomatic bradycardia and progression to CHB. For this reason, patients require hospitalization and evaluation for pacemaker placement.
2:1 Second Degree AV Block
It is important to highlight a specific scenario when there is 2:1 AV Block. In this case, it is difficult to determine if the AV Block is type I or type II, as there is no way to assess for P-R lengthening. In this situation, it is best to treat the patient as a type II AVB until proven otherwise.
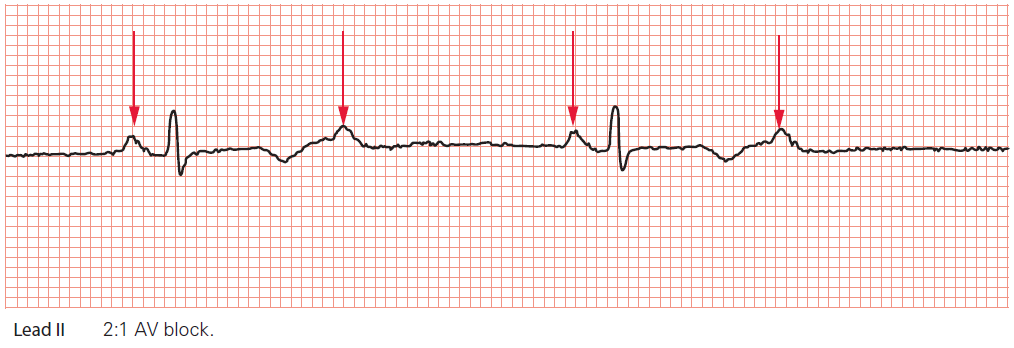
Key point: • The P waves are marked by arrows. Only every alternate P wave is followed by a QRS complex.
Read More about Conduction Blocks at the AV Node (AV Blocks)
ECG Cases of Second Degree AV Block:
- Atrial Tachycardia with 2nd degree AV Block – Mobitz I (Wenckebach)
- 3:2 Mobitz type II Second Degree AV Block
- Atrial Tachycardia with 3:2 AV Block Mobitz I Wenckebach
Key Points
- Mobitz type I AV Block is characterized by a lengthening P-R interval and a shortening R-R interval followed by a nonconducted P wave.
- Mobitz type I AV Block generally requires no treatment.
- Mobitz type II AV Block is characterized by a constant P-R interval with unpredictable nonconducted P waves.
- Mobitz type II AV Block is always abnormal and has high rate of progression to complete heart block.
- It is challenging to differentiate between type I and type II AV Block when conduction is in a 2:1 pattern.
Suggested Readings
- Josephson ME. Atrioventricular conduction. In: Clinical Cardiac Electrophysiology. 4th ed. Baltimore, MD: Wolters Kluwer, 2016:93.
- Langendorf R, Cohen H, Gozo EG. Observations on second-degree atrioventricular block, including new criteria for the differential diagnosis between type I and type II block. Am J Cardiol. 1972;29:111. https://pubmed.ncbi.nlm.nih.gov/4550168/
- Narula OS. Conduction disorders in the AV transmission system. In: Dreifus L, Likoff W, eds. Cardiac Arrhythmias. New York: Grune and Stratton, 1973:259.