This post is an answer to the ECG Case 243
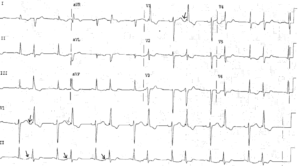
- Rate:
- Ventricular rate 42 bpm
- Atrial rate 105 bpm
- Rhythm:
- Regular ventricular rhythm
- Regular atrial activity
- No evidence of atrial to ventricular conduction
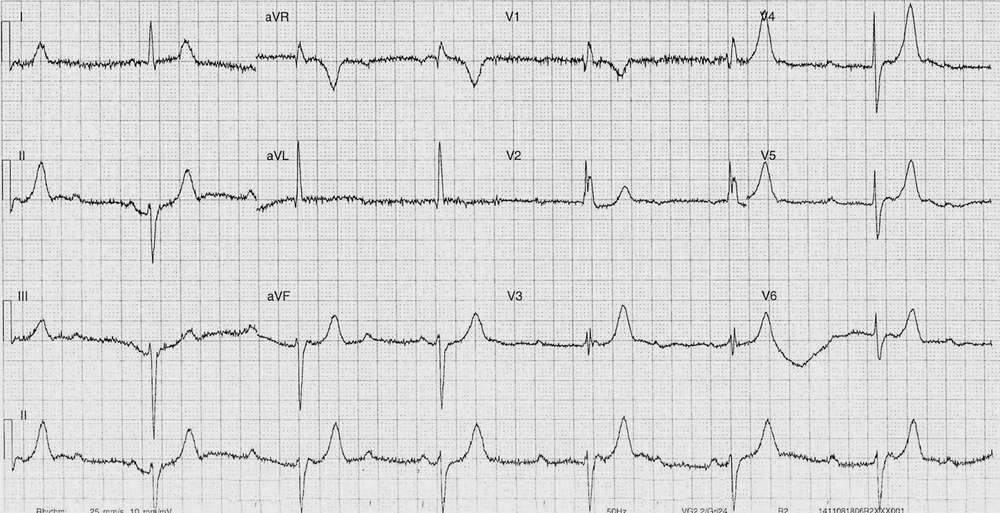
- Number of the P waves are buried in the T waves
- Atrial activity mapped out in image below

Dark green = visible P waves.
Light green = mapped location given fixed P-P interval
- Axis: LAD
- Intervals:
- QRS – Prolonged (120ms)
- QT – 460ms
- Segments:
- Possible ST elevation in leads aVR and V5-6
- Possible ST depression in lead V2
- Difficult to assess given baseline artifact and relative paucity of ventricular complexes seen in each lead
- Additional:
- RBBB Morphology
- Prominent T waves in leads I, II, aVF, V3-6
- Voltage criteria for LVH (aVL R wave >11mm)
- Baseline artifact
Interpretation
- Complete heart block
- Prominent T waves
- Hyperkalaemia ?
- Ischaemia ?
What happened next ?
There was no history of chest pain and the review of the her medications revealed only low dose calcium channel blocker use. Prior to this attendance she lived independently and alone with minimal prior medical history.
An old ECG on this patient showed long-standing RBBB and LAD in sinus rhythm without evidence of 1st degree AV block with similar T wave prominence as seen in this ECG.
An urgent venous blood gas show no hypo- or hyperkalemia and the rest of her electrolytes, renal function and serial troponins were normal. She was admitted to CCU on an isoprenaline (isoproterenol) infusion and had a pacemaker inserted without complication.
READ MORE:
SIMILAR CASE: Complete (third degree) Heart Block in 80-year-old woman