This post is an answer to the ECG Case 257
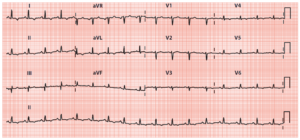
- Rate:
- Ventricular rate 42 bpm
- Atrial rate 84 bpm
- Rhythm:
- Irregular atrial activity
- Short P-P (Green) followed by long P-P (Red) – see image below
- The shorter P-P interval occurs when a ventricular (QRS) complex occurs between the P waves whilst the longer P-P interval occurs when there is no ventricular (QRS) complex between the P waves
- This phenomenon is known as Ventriculophasic Arrhythmia
- 2:1 AV Block with ventricular (QRS) complexes only occurring after every second P wave

- Axis: LAD
- Intervals: QRS – Prolonged (160ms)
- Segments: Subtle ST elevation leads II, III, aVL
- Additional: RBBB Morphology
Interpretation
- 2:1 2nd Degree AV Block
- Bifascicular block
- RBBB + LAFB
- Ventriculophasic Sinus Arrhythmia
- Symptomatic Patient with syncope
What happened next ?
The patient was referred to the cardiology team and had an uneventful PPM insertion.
What is Ventriculophasic Sinus Arrhythmia ?
This ECG is a nice example of ventriculophasic arrhythmia, this phenomenon can be seen in up 40% of cases of complete AV block and, as in this case, can be seen with 2nd degree AV block also.
You get a shorter P-P interval when there is an associate QRS complex with a longer P-P when there is no QRS between the P waves.
Several mechanisms have been proposed including alterations in sinus node perfusion related to ventricular contraction and the mechanical effects of atrial stretch. To make things more confusing there is a much rarer paradoxical phenomenon when the P-P is longer when a QRS is contained between them. It is important to recognized as the P-P variability may be mistaken for other ECG features such as U waves for example.
READ MORE: