This post is an answer to the ECG Case 266
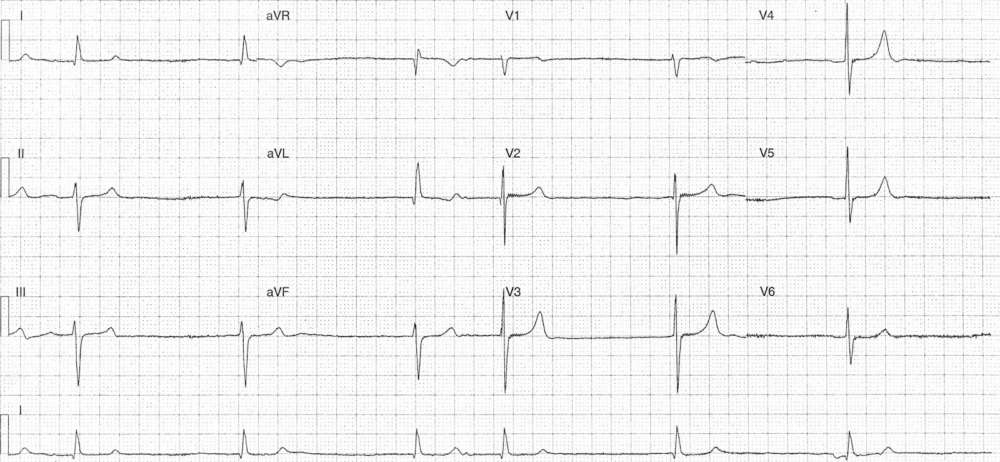
- Rate: 36 bpm
- Rhythm:
- Irregular
- No consistent atrial activity
- Possible atrial activity in ST segment of 2nd complex and after T wave of 3rd complex
- Axis: LAD
- Intervals:
- QRS – Normal (100ms)
- QT – 480ms (QTc Bazette 375 ms)
- Additional:
- T waves in leads V3-5 appear prominent and peaked
Interpretation
- Slow atrial fibrillation
- Broad differentials include:
- Drug toxicity
- Sinus node dysfunction
- Hypothermia
- Electrolyte abnormalities
- Ischaemia
What happened next ?
The patient had taken an extra metoprolol dose earlier in the day. Venous blood gas revealed a potassium of 7.0 mmol/L. Further beta-blocker medication was withheld and hyperkalaemia was treated with calcium gluconate and insulin / dextrose therapy prior to planned dialysis later in the day. Following ED treatment of hyper-k the patients heart rate improved to ~50 bpm and he made an uneventful recovery.