This post is an answer to the ECG Case 297
- Rate: 66 bpm
- Rhythm: Sinus arrhythmia
- Intervals:
- PR – Normal (~180ms)
- QRS – Normal (110ms)
- QT – 400ms (QTc Bazette 420 ms)
- Segments:
- ST elevation in leads I (<1mm), aVL (0.5-1mm), V1 (<1mm), V2-3 (1mm)
- ST depression in lead III, aVF
- Additional:
- P wave prolonged 110ms and notched in lead II consistent with left atrial abnormality
- Poor R wave progression in precordial leads
- T wave inversion in leads III and aVF
- R wave aVL ~11mm – LVH voltage criteria
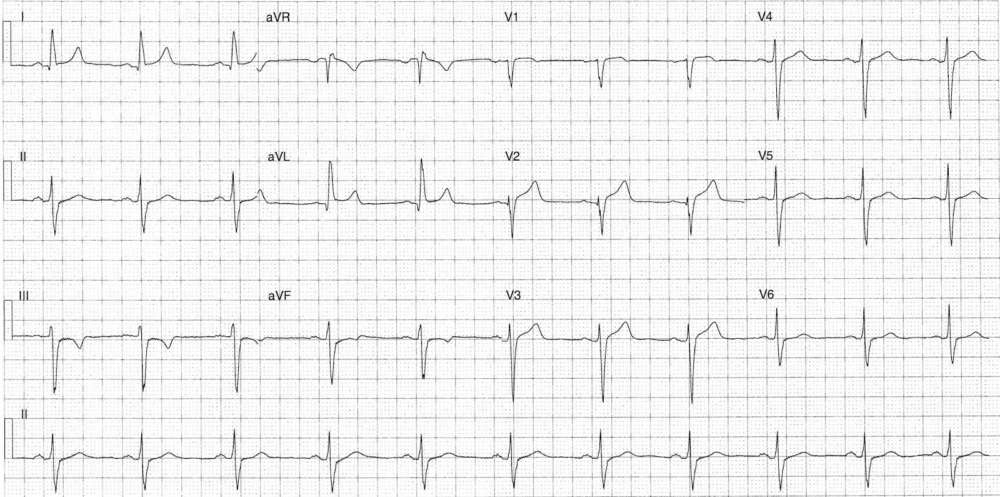
Interpretation
Sinister features for ACS include T wave inversion in inferior leads and ST elevation in high lateral leads (I, aVL) and right precordial leads (V1-3)
What happened next ?
Initial troponin was elevated at 5.69 (cTnI [<0.05 ug/L]). The patient was admitted under cardiology and had an angiogram which showed:
- LMCA: Normal
- LAD: 30-40% stenosis mid and distal
- Cx: Irregularities
- RCA: 30-40% stenosis mid vessel
- 2nd OM: 100% occlusion with RCA collaterals – DES inserted
Post angio echo showed:
- EF 52%
- Hypokinesis of lateral wall of left ventricle
- Moderate concentric left ventricular hypertrophy
The patient was discharged on dual anti-platelet therapy (DAPT), beta-blocker, statin and ACE.