This post is an answer to the ECG Case 318
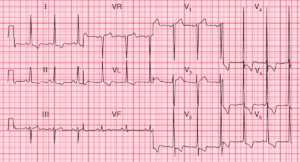
- Rate: 54 bpm
- Rhythm: Regular sinus rhythm
- Axis: Normal
- Intervals:
- PR – Normal (~120ms)
- QRS – Normal
- QT – 420ms
- Segments:
- ST Elevation in leads aVR, V1-2
- ST Depression in leads II, aVF, V4-6
- Additional:
- Deep T wave inversion leads V2-6
- Terminal positive deflection to T wave in these leads ?U wave
- T wave inversion in leads I, II, aVF
- Massive R waves in all precordial leads
- Deep T wave inversion leads V2-6
Interpretation
Extensive T wave abnormalities with massive precordial QRS complexes
The differential for these ECG features given the clinical scenario would be:
- Electrical injury related
- Incidental finding of cardiomyopathy ( ECG pattern favours apical variant)
What happened next?
On history review the patient had no history of loss of consciousness, syncope, palpitations or chest pain related to his presenting injury. There was a positive family history of cardiomyopathy in a close relative but no history of sudden cardiac death. The patient was admitted under cardiology for further investigation. The patient had negative serial troponins and underwent angiogram which showed:
- Normal coronary arteries
- Normal LV function
- Apical hypertrophy
Subsequent echo showed:
- Normal LV cavity size and function
- Asymmetric distribution of left ventricular hypertrophy affecting the apical LV region
The patient’s investigation findings are consistent with apical hypertrophic cardiomyopathy, sometimes referred to as Yamaguchi Syndrome. He was discharged with ongoing cardiology follow-up.
SIMILAR CASE: ECG Case 268