ECG Interpretation
- Sinus rhythm, rate 71/min
- Normal axis
- Tall R waves and deep S waves in the chest leads
- ST segment depression in leads I, II, VL, V3–V6
- Inverted T waves in leads I, II, VL, V3–V6 (Left ventricular strain pattern)
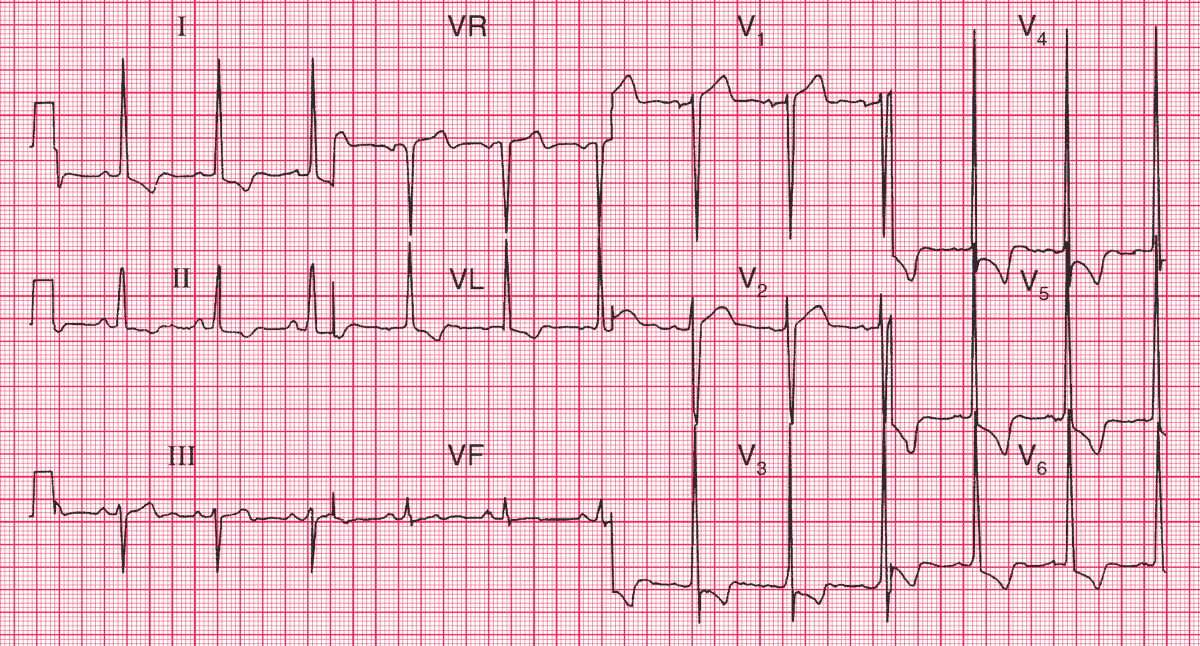
Clinical interpretation
This is marked left ventricular hypertrophy. It can be difficult to distinguish between T wave inversion due to ischaemia and the T wave inversion of left ventricular hypertrophy, and when the T wave is inverted in the septal leads (V3–V4), ischaemia has to be considered.
However, here the change is most marked in the lateral leads, and is associated with the ‘voltage criteria’ for left ventricular hypertrophy.
READ MORE: Left Ventricular Hypertrophy (LVH): How to Recognize it on ECG [With Examples]
Angina, dizziness and left ventricular hypertrophy in an 85-year-old may be due to tight aortic stenosis, though hypertension is a possibility.
What to do ?
Look for the signs of aortic stenosis (‘plateau’ pulse, narrow pulse pressure, displaced apex beat, aortic ejection systolic murmur) and confirm the valve gradient with echocardiography.
In this patient the aortic valve gradient was 20 mmHg, indicating trivial stenosis of the valve, so the left ventricular hypertrophy must be due to the long-standing hypertension.
The angina may well improve with adequate blood pressure control and the usual anti-anginal medication, but if it does not, then 85 years is not too old for coronary angiography with a view to percutaneous coronary intervention (PCI) or bypass surgery.