The rhythm is regular at a rate of 130 bpm. The QRS complex is wide (0.20 sec). The QRS morphology is abnormal and does not resemble either a typical right or left bundle branch block.
Although no obvious P waves are seen before any of the QRS complexes, there is evidence of atrial activity (+), best seen in the lead VI rhythm strip, for example, before the second, seventh, 12th, and 17th QRS complexes and after the third, eighth, 13th, and 18th QRS complexes (note the positive waveform at the end of the T wave that is not seen with the other QRS complexes).
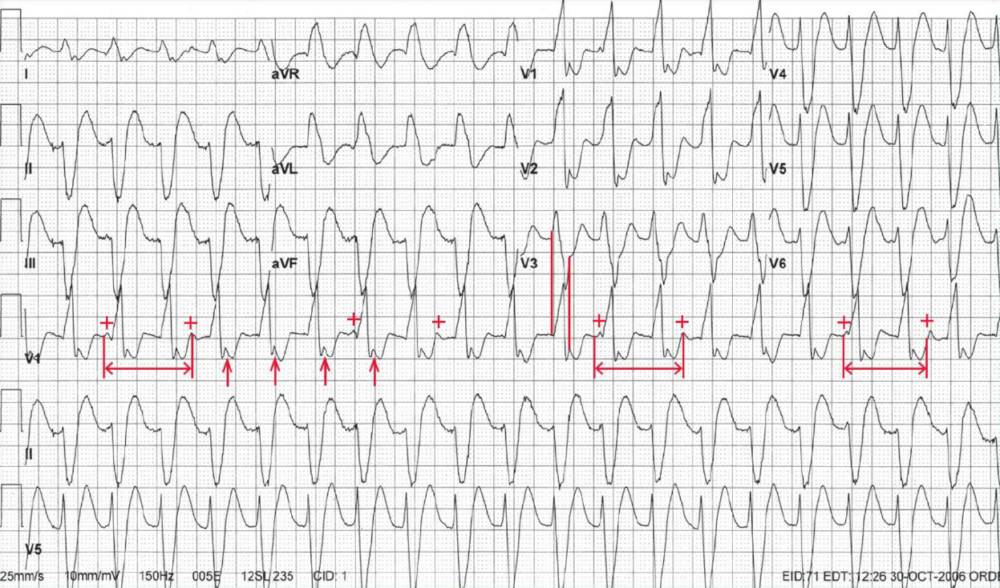
It should be noted that the positive waveform that appears to be present after the QRS complex in leads V1-V2 (↑) is not a P wave but is actually part of the QRS complex. This can be established by measuring the maximum QRS complex width (eg, in lead V3) and comparing this with the QRS complex width in leads V1-V2 (||).
There is no relationship between the P waves and the QRS complexes (ie, the PR intervals are variable without any pattern); therefore, this is AV dissociation.
It is not necessary that the P waves “march out” completely to make the diagnosis of AV dissociation, but rather that there are P waves associated with some (but not all) of the QRS complexes.
The atrial rate is about 72 bpm, which can be established by the fact that whenever two sequential P waves are seen (<->) the rate is identical at 72 bpm.
A wide complex tachycardia associated with AV dissociation and an atrial rate that is slower than the ventricular rate (ie, an enhanced lower focus) is characteristic of sustained ventricular tachycardia. As all the QRS complexes are similar, this is termed monomorphic ventricular tachycardia.
AV dissociation occurs because the ventricular complex conducts into the AV node but does not get through to activate the atrium. However, it does totally depolarize the node, causing it to be completely refractory and preventing antegrade conduction of the sinus complex. Since the ventricular impulse does not reach the atrial myocardium, the sinus node is not depressed or overdriven.