This post is an answer to the Case – 2-year-old Boy with Fever, and ‘Brassy’ Cough
What radiological abnormalities are seen ?
The characteristic ‘steeple sign’ of the subglottic trachea with loss of the normal shoulders.
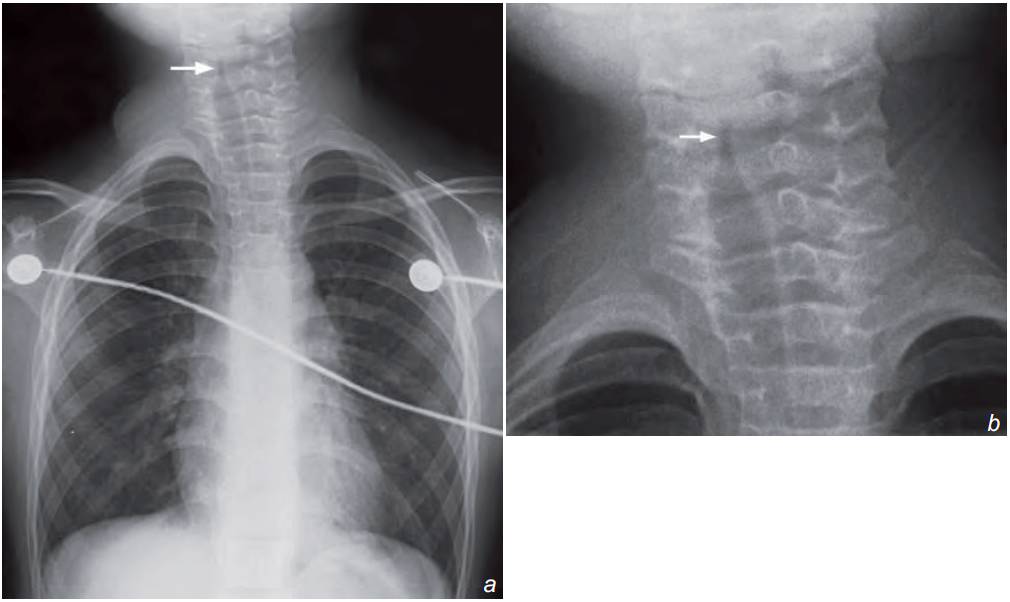
Chest x-ray shows characteristic subglottic inverted v ‘steeple sign’ with loss of the normal shoulders (arrow). CXR also helps to exclude foreign body inhalation as a cause of acute stridor.
Discussion
Croup/laryngotracheobronchitis is inflammation of the respiratory tract, usually viral in nature. It is the most common cause of acute stridor in children between 6 months and 3 years of age. However, it may also occur in older children and adults.
All the mucosa along the respiratory tract from the larynx to the bronchi are involved and oedematous. The subglottic area becomes the part critically compromised as the mucosa here is loosely attached
Other radiological findings of croup/laryngotracheobronchitis include:
- Distension of the hypopharynx on lateral view of neck
- Indistinctness of the subglottic airway with normal epiglottis and normal aryepiglottic folds on a lateral view
- Radiographs also help to exclude foreign body inhalation as a cause of acute stridor.
READ MORE: Stridor in Children – Diagnostic Algorithm and Treatment
SIMILAR CASE: 1-year-old Boy with 3-day History of Fever, Cough, and Hoarseness