
This post is an answer to the Case – 28-year-old Woman with Asthma and Worsening Dyspnea
Findings
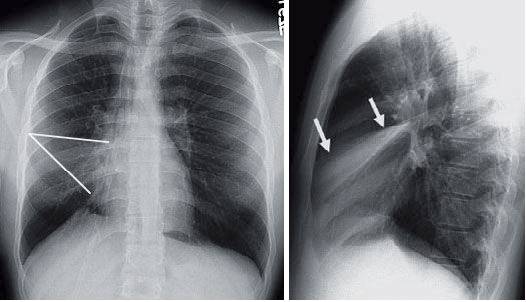
- Initial frontal radiograph contains a vague triangular opacity that effaces the right heart border (overlay). Accompanying volume loss is best appreciated by the effect on the right hemidiaphragm.
- On the lateral radiograph, the lobar collapse is seen as a dense triangle with a central apex and the base against the anterior chest wall. The superior border is made up by the horizontal (minor) fissure (arrows) and the inferior edge by the major fissure. The orientation of the minor fissure explains why it is no longer clearly seen on the frontal radiograph.
Differential Diagnosis
Right middle lobe collapse and right middle lobe consolidation from pneumonia are the two main considerations. The volume loss strongly supports the former.
Teaching Points
- Right middle lobe collapse is the lobar collapse least associated with volume loss as it is the lobe with the least volume.
- Early collapse is associated with effacement of the right heart border known as the silhouette sign.
- As the collapse progresses, it pulls the minor fissure inferiorly out of the transverse plane. The net effect is that the minor fissure is no longer well seen on the frontal projection.
- The lateral radiograph is characteristic for right middle lobe collapse. The volume loss results in approximation of the major and minor fissures with a resultant dense triangle over the heart.
- Rarely, right middle lobe collapse may be longstanding as a result of chronic inflammation, bronchiectasis, or fibrosis. The term right middle lobe syndrome has been used to refer to chronic nonobstructive, right middle lobe collapse.
Management
- With simple collapse, the management rests on pulmonary toilet and occasional bronchoscopy to clear the mucus.
- With a central mass, the treatment is aimed towards diagnosing the mass, usually by bronchoscopic biopsy, and then surgical resection, if possible.
Further Reading
Woodring, John H. M.D.; Reed, James C. M.D.. Radiographic Manifestations of Lobar Atelectasis. Journal of Thoracic Imaging 11(2):p 109-144, Spring 1996.
