This article is an answer to the Case – Patient with Absence of Breath Sounds in the Right Hemithorax
Chest radiography performed at emergency department revealed an opaque right hemithorax and a mediastinum entirely displaced to the right side. The trachea was also displaced to the right and the left main bronchus is depicted; however, the right main bronchus is not seen.
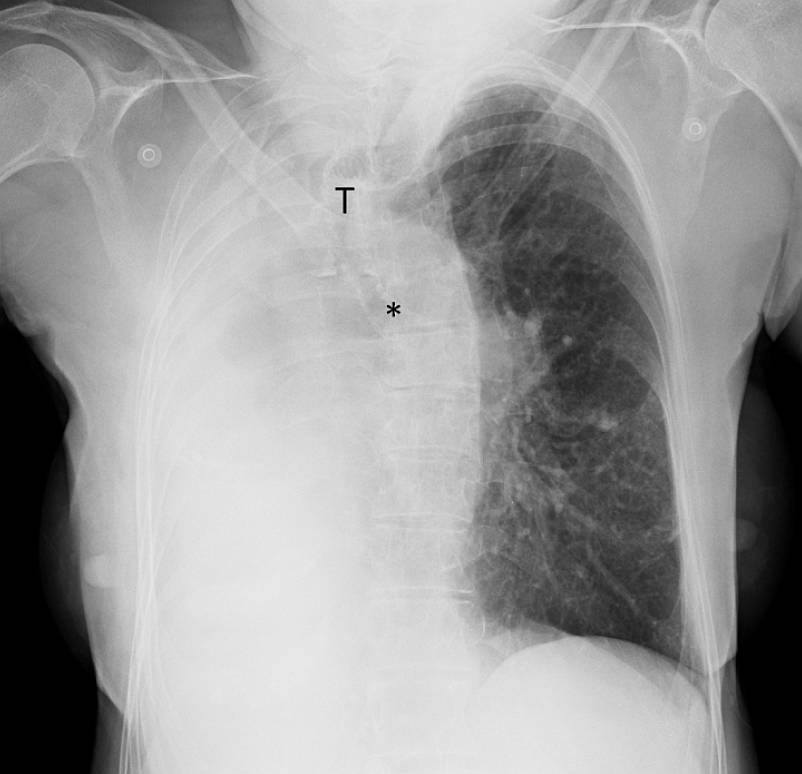
The right intercostal spaces seem reduced relatively to the left ones, indicating volume reduction; the left lung appears radiolucent due to compensatory overinflation.
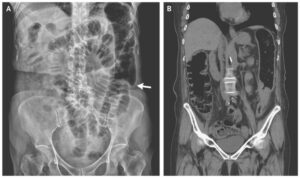
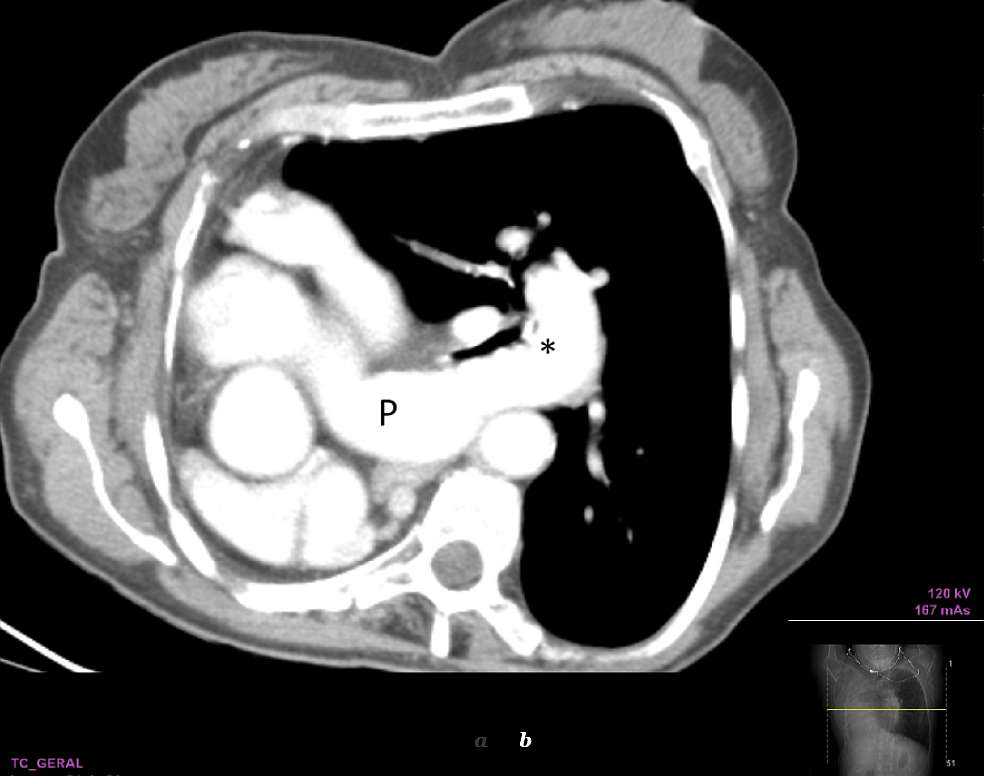
She underwent a CT scan, which showed a complete absence of the right lung, a normal hyperinflated left lung and a clear shift of the mediastinum to the right (dextrocardia). Absence of the right pulmonary artery and of the right main bronchus was also shown.

Differential Diagnosis List
- Unilateral pulmonary agenesis
- Total atelectasis from any cause
- Pneumonectomy
- Pulmonary aplasia or hypoplasia
- Lung infection/pneumonia
- Diaphragmatic hernia
- Severe bronchiectasis with collapse
- Advanced fibrothorax
Discussion
Unilateral pulmonary agenesis is a rare congenital malformation with an incidence of 1:10,000-15,000 [1, 2]. Pulmonary agenesis is part of the lung agenesis-hypoplasia complex (lung underdevelopment) and consists of a complete absence of lung parenchyma, its bronchus and vascular supply [1, 3].
The aetiology of pulmonary agenesis remains unknown. Genetic, teratogenic, and mechanical factors, notably abnormal blood flow in the dorsal aortic arch during the 4th week of gestation, have been proposed as possible causes [1, 3-5].Associated malformations and the location of the missing lung are the main prognostic determinants. More than 50% of cases have associated congenital anomalies that involve the cardiovascular, gastrointestinal, musculoskeletal, and genitourinary systems [1, 3]. The disorder occurs on either side with almost equal frequency [6]. Patients with right lung agenesis have a shorter life expectancy [3], related to a more severe mediastinal and cardiac displacement and greater frequency of associated cardiac anomalies [1-3].
The clinical presentation depends on the degree of pulmonary abnormality and the presence of other congenital malformations. In some cases, symptoms manifest at birth as respiratory distress syndrome. In others, patients remain asymptomatic until adulthood, when lung agenesis can be an incidental finding [1, 6]. If not complicated by other abnormalities, patients are usually asymptomatic, do not require intervention and can have a normal life [1].
Imaging studies are essential for the diagnosis of pulmonary agenesis. The diagnosis is usually first suspected on chest radiography, which demonstrates a diffuse opacity of the affected hemithorax and an ipsilateral mediastinal shift [1, 6, 8]. A normal contralateral lung with compensatory hyperinflation and herniation across the midline is a common finding [6]. CT confirms the absence of lung parenchyma, pulmonary artery, and bronchial structures on the affected side [4, 6, 7]. CT angiography and MR angiography are currently the imaging modalities of choice in the diagnosis of this entity [6].
Other ancillary tests, such as echocardiography to rule out cardiac anomalies may be indicated [1].There are few case reports regarding patients with right lung agenesis living to old age because of both severe mediastinal and cardiac displacements [8]. Our patient didn´t have other thoracic abnormalities, besides dextrocardia, which probably explains the previous unawareness of this anomaly.
References
- Malcon MC, Malcon CM, Cavada MN, Caruso PEM, Real LF. (2012) Unilateral pulmonary agenesis. J Bras Pneumol 38(4): 526-529. (PMID: 22964938)
- Gokhan GA, Ozbilim G, Bozova S, Gra A, Ongun H, Michi E, Arslan G. (2005) Unilateral pulmonary agenesis associated with colloidal goiter in a newborn: a case report. Turkish J Ped 48: 295-297. (PMID: 16250321)
- Berrocal T, Madrid C, Novo S, Gutiérrez J, Arjonilla A, Gómez-León N. (2004) Congenital anomalies of the tracheobronchial tree, lung, and mediastinum: embryology, radiology, and pathology. RadioGraphics 24(1): e17. Epub 2003 Nov 10. (PMID: 14610245)
- Biyyam DR, Chapman T, Ferguson MR, Deutsch G, Dighe MK. (2010) Congenital lung abnormalities: embryologic features, prenatal diagnosis, and postnatal radiologic-pathologic correlation. RadioGraphics 30(6): 1721-38. (PMID: 21071385)
- Zylak CJ, Eyler WR, Spizarny DL, Stone CH. (2002) Developmental lung anomalies in the adult: radiologic-pathologic correlation. RadioGraphics 22 Spec No: S25-43. (PMID: 12376599)
- Lee EY, Boiselle PM, Cleveland RH. (2008) Multidetector CT evaluation of congenital lung anomalies. Radiology 247(3):632-48. (PMID: 18487532)
- Daltro P, Fricke BL, Kuroki I, Domingues R, Donnelly LF (2004) CT of congenital lung lesions in pediatric patients. AJR 183(5):1497-506. (PMID: 15505327)
- Ueda T, Nozoe M, Nakamoto Y, Irie Y, Mizushige K. (2011) Right Pulmonary Agenesis in an Elderly Woman Complicated by Transient Ischemic Attack. Inter Med 50(5):463-6. (PMID: 21372460)