This post is an answer to the ECG Case 231
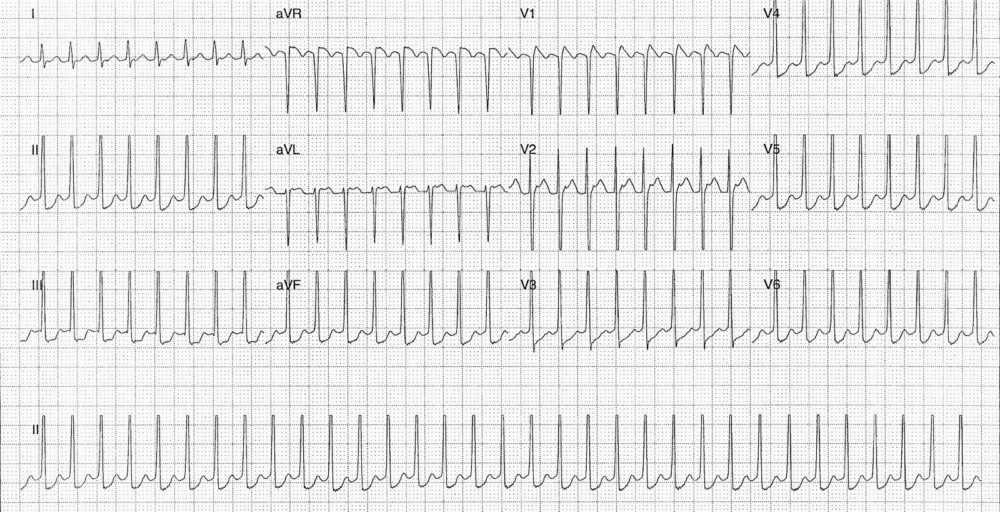
- Rate: ~200 bpm
- Rhythm: Regular
- Axis: Normal axis
- Intervals:
- QRS – Normal (600ms)
- QT – 220ms (QTc Bazette415 ms)
- Segments:
- ST Elevation in leads aVR, V1, V2
- ST Depression in leads II, III, aVF, V3-6
- Additional:
- Retrograde p waves best visible in leads aVL and V2
- Pseudo-R prime & Pseudo S
- Retrograde p waves best visible in leads aVL and V2
Interpretation
- Narrow Complex Tachycardia in a paediatric patient.
- AVNRT
- The retrograde P wave in V1, V2 is too close to the QRS to be AVRT
- You can not make it from ventricle to atrium over an accessory pathway so quickly you need a minimum of 70-80 msec
What happened next ?
A venous blood gas revealed normal electrolytes. Vagal manoeuvres were attempted but failed to revert the rhythm so we proceeded to adenosine. A 100 mcg/kg dose resulted in successful cardioversion.
Management of Paediatric SVT
90% of paediatric arrhythmias are SVT. 90% of SVTs are of re‐entrant type. Half of paediatric patients with SVT will have no underlying heart disease, a quarter will have congenital heart disease and the other quarter will have Wolf Parkinson White syndrome.
Look for potential precipitants such as fever, metabolic/electrolyte abnormalities, and drug exposure. The SVT may be well tolerated for an extended period, up to 12-24 hours before signs of cardiac failure appear.
Treatment should occur in a step-wise manner. In the uncomplicated patient vagal maneuvers should be tried prior to chemical cardioversion, with adenosine being the preferred agent. If chemical cardioversion with adenosine is unsuccessful paediatric cardiology advice should be sought for advice on next-line agents. For complex patients early paediatric cardiology advice should be sought.
Options for vagal maneuvers depend on patients age. For Infants you can put iced water in bag and place this on the face for up to 10 seconds. In older children you can try carotid sinus massage, valsalva , deep inspiration/cough/gag reflex, and even headstand.
Adenosine is a very short acting AV and sinus nodal blocker. It is given via a proximal IV cannula followed by / or with a saline flush. Side-effects are transient but including flushing, nausea, bronchospasm, and ‘sense of doom’. It is given in an escalating dose regime:
- 1st dose 100 mcg/kg
- 2nd dose 200 mcg/kg
- 3rd dose 300 mcg/kg
- Give doses 2 minutes apart.
- Maximum single dose 12mg
Do NOT use verapamil or beta blockers in infants or children with SVT – cause profound AV block, negative inotropy and sudden death.
The shocked / compromised child with SVT will require DC cardioversion. Be very wary of cardioverting an ‘unstable’ child in a SVT who requires sedation or anaesthesia as rapid deterioration of the ‘SVT‐stressed’ myocardium may occur with anaesthesia with resultant death.
READ MORE: Never Mistake Ventricular Tachycardia for Supraventricular Tachycardia with Aberrant Conduction
SIMILAR CASES: