This article is an answer to the ECG Case 158
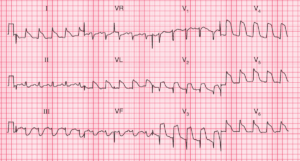
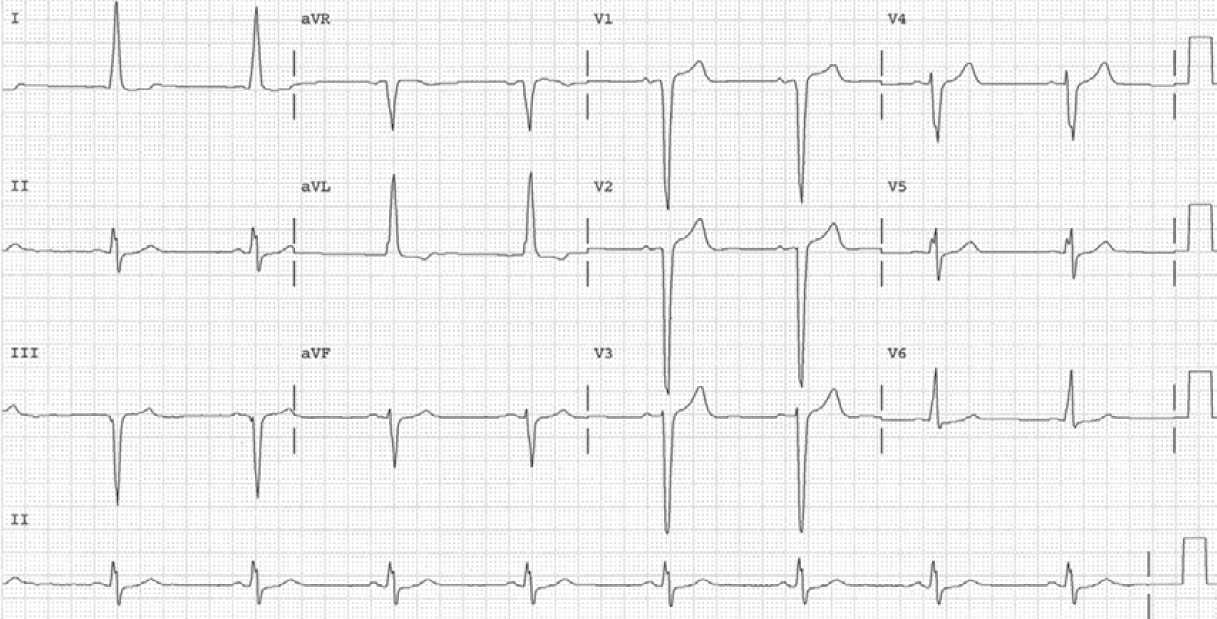
The ECG shows a regular rhythm at a rate of 150 bpm. There are no P waves seen before or after any of the QRS complexes. The QRS complex duration is increased (0.16 sec), and hence this is a wide complex tachycardia, which may be either ventricular tachycardia or a supraventricular tachycardia with aberration.
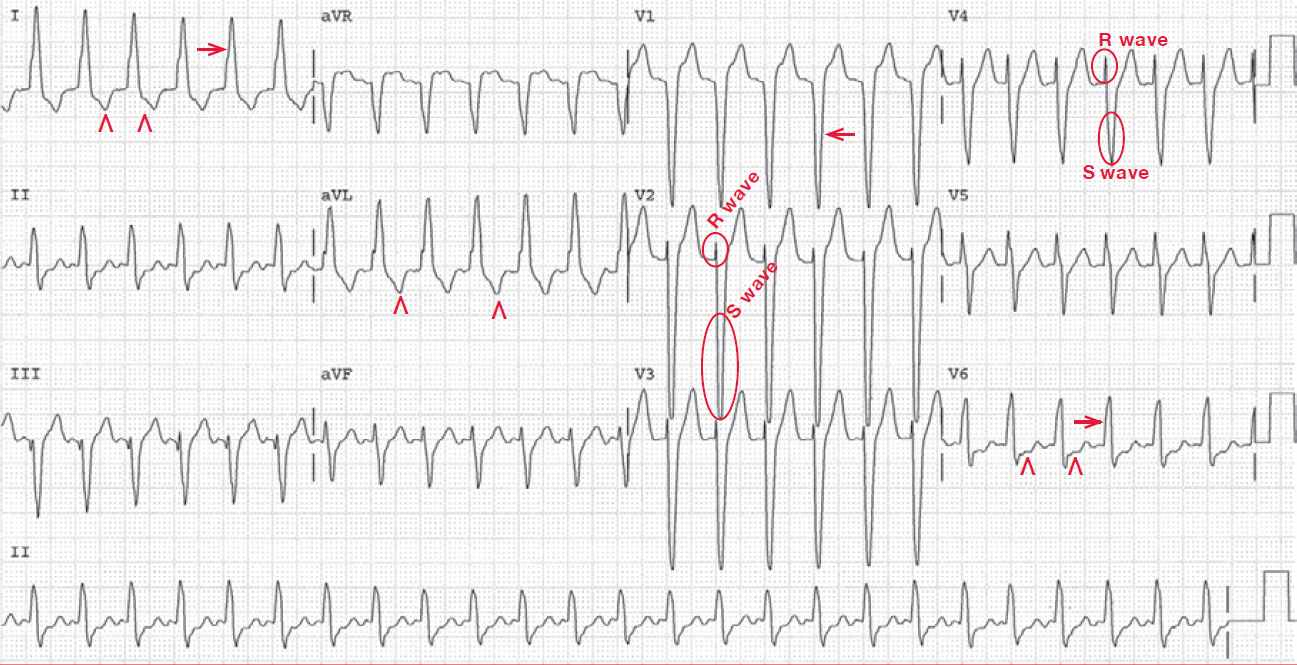
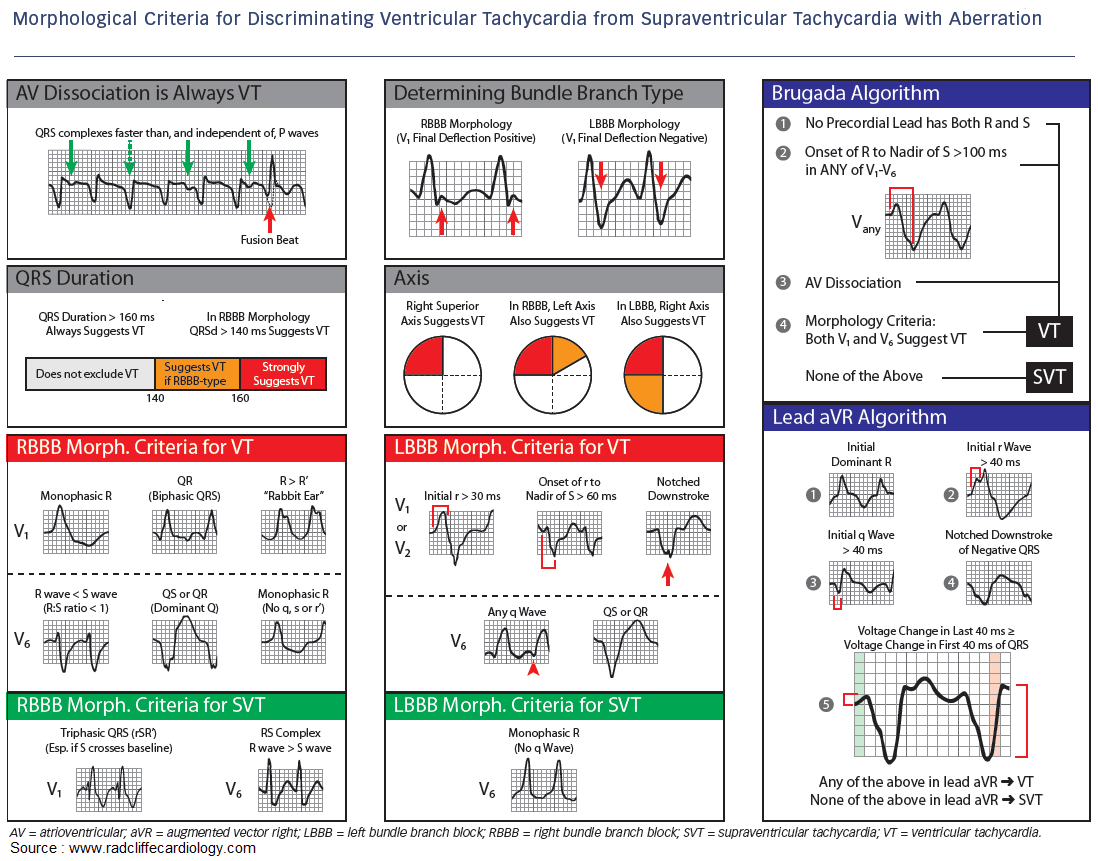
The morphology is that of a typical left bundle branch block with a tall, broad R wave in lead I (→) and V6 and a deep QS complex in lead V1 (←). There are ST-T wave changes seen in leads I, aVL, and V6 (^). If this is a left bundle branch block, then these are secondary to the left bundle branch block. If this is a ventricular tachycardia, then the T-wave abnormalities reflect the presence of a ventricular complex.
It is not clear from this ECG if this is a supraventricular tachycardia or a ventricular tachycardia. However, there are R/S complexes in leads V2–V4, the R wave is wider than the S wave (R/S < 1), and the R wave is less than 100 msec. As the initial forces are normal, while it is the terminal portion of the QRS complex that is wide, this morphology is consistent with a supraventricular tachycardia with a left bundle branch block aberrancy.
The absence of recognizable P waves establishes this as a no-RP tachycardia and the most common arrhythmia presenting in this fashion is an atrioventricular nodal reentrant tachycardia.
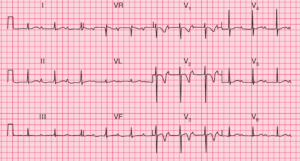
The following ECG recorded her heart rate has slowed shows sinus rhythm with LBBB, so this confirms that the diagnosis of the previous ECG was indeed AVNRT with aberrancy (LBBB).
- READ MORE:
- SIMILAR CASES: