There is a regular rhythm with a rate of 52 bpm. There is no P wave seen before or after any QRS complex. The QRS complex duration is normal (0.10 sec), best measured in lead V4, and the morphology is normal. Therefore, this is a junctional rhythm.
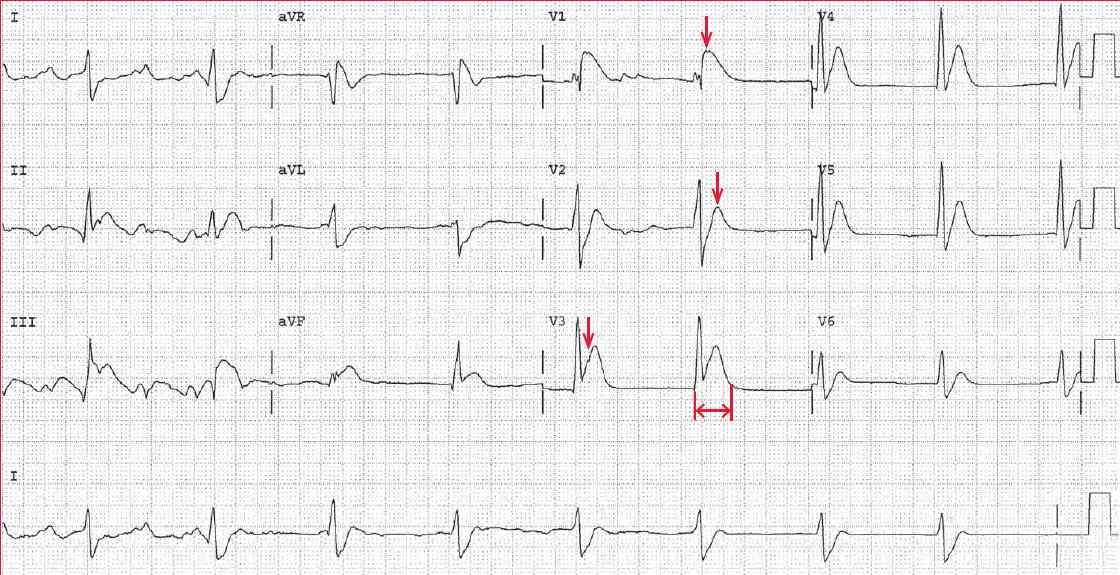
The axis is normal between 0° and +90° (positive QRS complex in leads I and aVF). The QT interval (↔) is 0.34 sec, and when corrected for heart rate, the QTc is 0.32 sec and hence very short. This is due to the absence of any ST segment. In addition, there is the appearance of ST-segment elevation and an acute myocardial infarction, particularly in leads V1–V3 (↓).
A short QT interval (defined as a QTc ≤ 0.34 sec) is due to metabolic abnormality (high calcium or magnesium) or a congenital short QT syndrome that is due to a channelopathy involving the sodium, potassium, or calcium channels. The congenital short QT syndrome is associated with an increased risk of sudden death due to ventricular fibrillation.
In this case, the short QT interval is the result of hypercalcemia, which is due to multiple myeloma. Usually there are no arrhythmic problems associated with hypercalcemia.
ST-segment elevation mimicking myocardial infarction has been reported with hypercalcemia; it is seen in this patient. It is likely that the apparent ST segment elevation is actually the T wave that is at the very end of the QRS complex as a result of the short ST segment.