
This post is an answer to the Case – Patient with Dyspnoea and Dysphagia for Several Years
Physical examination revealed a diffusely enlarged thyroid with palpable nodules up to several centimetres. The lower edge of the thyroid gland was not palpable.
Imaging Findings
A posteroanterior chest radiograph showed a giant posterior mediastinal mass causing anterior deviation of the trachea (Fig. 1). Lateral chest radiograph showed posterior displacement of the aorta and anterior deviation of the pulmonary hilum by the mass. Narrowing of the intermediate bronchus was also noted.

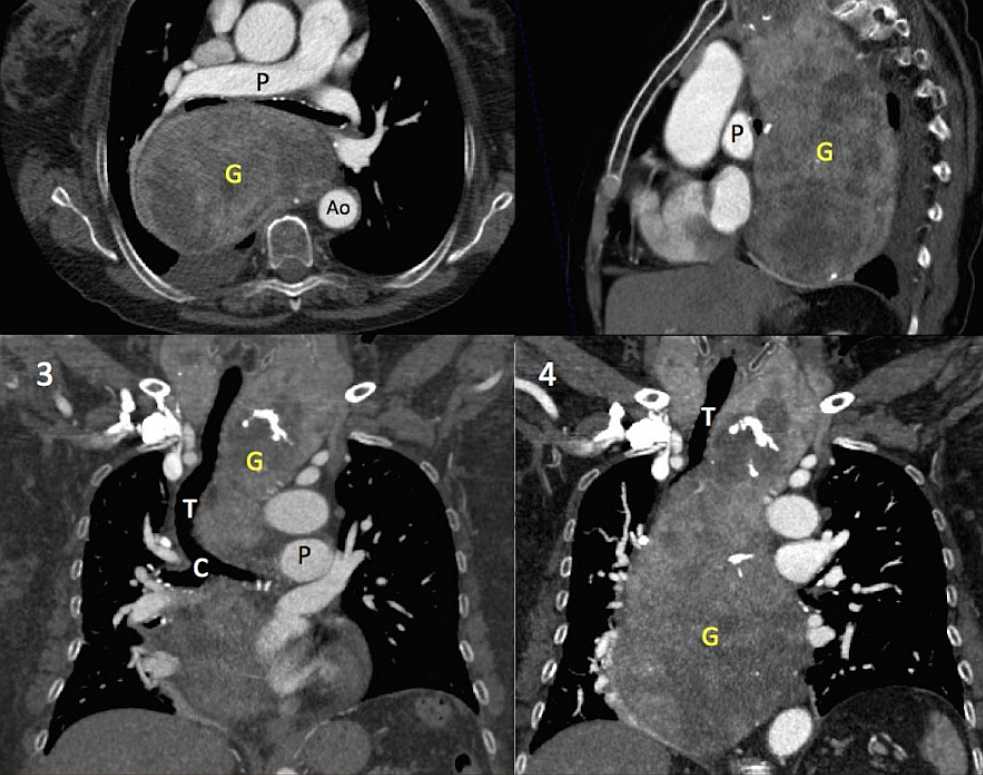
A contrast-enhanced chest CT revealed a large heterogeneously enhancing soft tissue mass (20 x12x9 cm) with calcifications extending from the cervical region to the right hemidiaphragm (white arrows in figure 2.2 and 2.4). It caused compression and deviation of the trachea, carina, oesophagus and vascular structures.
Surgery was performed via cervical and thoracic approach, and a large mass weighing 780 gr was resected. Pathological results were consistent with a thyroid goitre.
SIMILAR CASE: Mediastinal Extension of a Goiter


