This post is an answer to the ECG Case 269
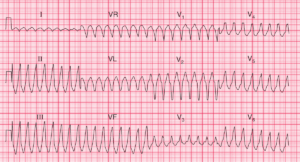
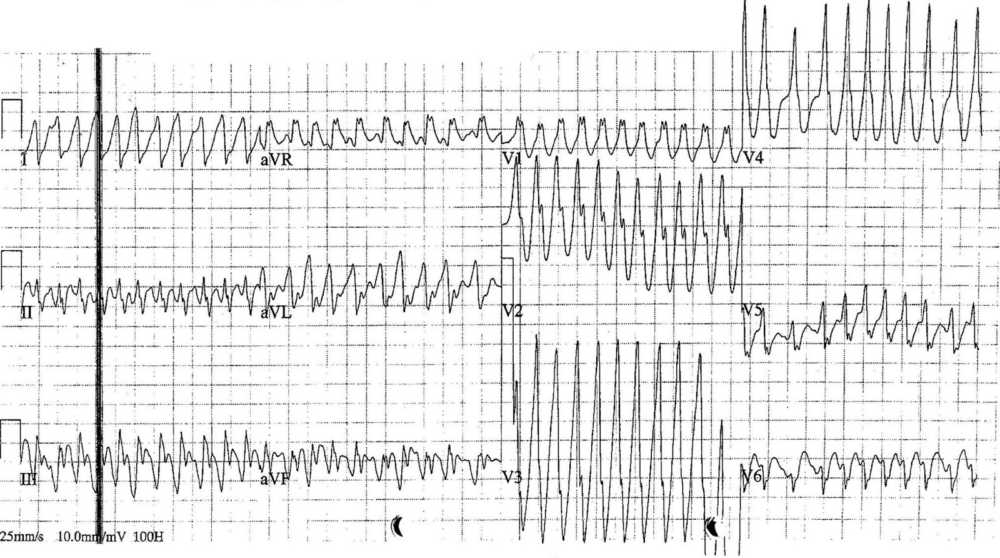
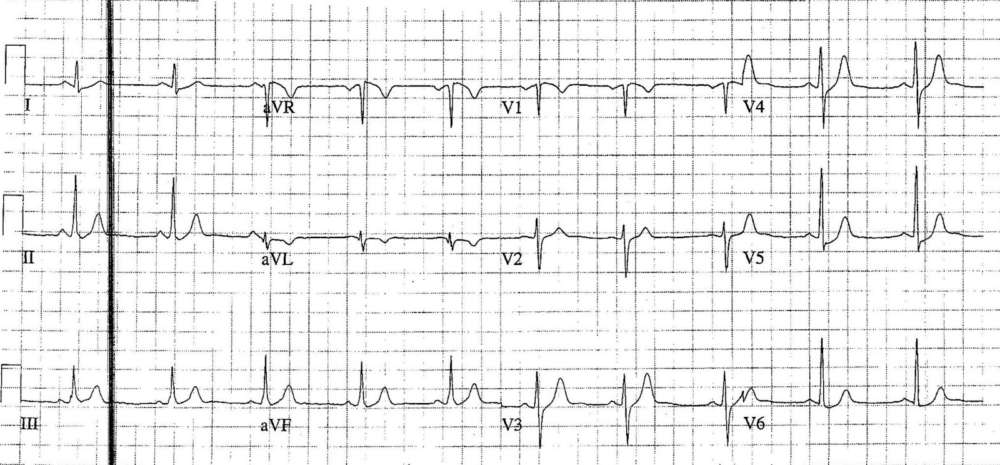
- Rate:
- Mean ventricular rate ~260 bpm
- Variable rate up to 300 bpm
- Rhythm: Irregular rhythm
- Axis: Indeterminate
- Intervals: QRS – Broad with variable width
- Additional: RBBB Morphology in lead V1
Interpretation
Atrial Fibrillation in the setting of pre-excitation / WPW
- Irregular
- Very fast
- Variable QRS width
Why is this rhythm important ?
This is a clinical situation in which significant harm to the patient can occur if the ECG features are not recognised and acted on appropriately. The concern with pre-excited AF is the ability for the accessory pathway to conduct at much higher rates than the AV node with the potential for degeneration into ventricular fibrillation.
It is for this reason that any drugs which block the AV node are ABSOLUTELY CONTRAINDICATED in this scenario including adenosine, calcium-channel blockers, beta-blockers and digoxin. If the AV node is blocked then there is increased conduction via the accessory pathway which may precipitate ventricular fibrillation. Put simply if you give the patient AV nodal blocking drugs you might kill them.
The safest and easiest method to restore sinus rhythm is synchronised cardioversion. Chemical cardioversion is a possible alternative in stable patients with iv procainamide being the commonly used agent.
What happened next?
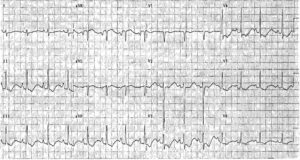
The patient underwent synchronised DC cardioversion and his post cardioversion ECG is below.
READ MORE: Atrial Fibrillation in the Wolff-Parkinson-White (WPW) Syndrome
SIMILAR CASES: