This post is an answer to the ECG Case 300
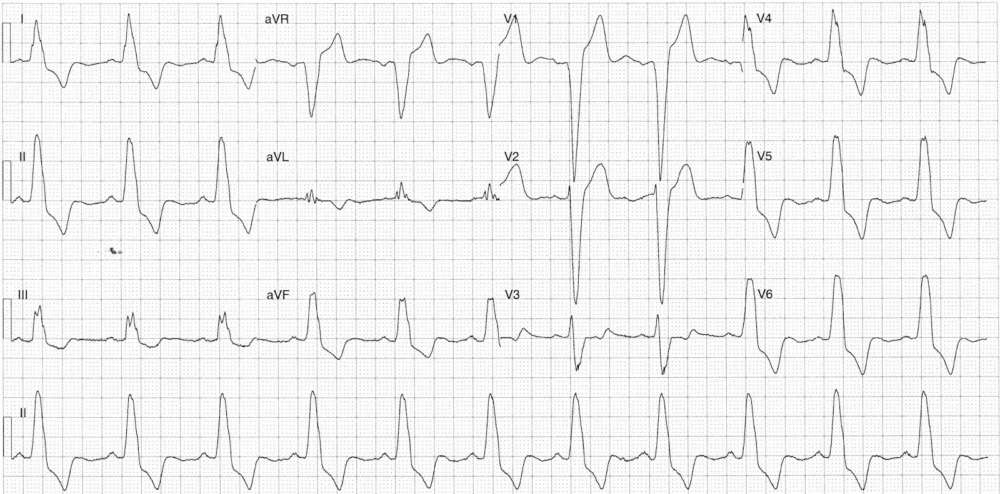
- Rate: 66 bpm
- Rhythm: Regular sinus rhythm
- Axis: Normal
- Intervals:
- PR – Normal (~180ms)
- QRS – Prolonged (200ms)
- QT – 400ms (QTc Bazette 380-400 ms)
- Segments / Additional:
- LBBB
- Discordant ST segment change with appropriate magnitude
- See the Smith paper below for an explanation of ‘excessive’ discordance
- Lead V3 looks concerning for ACS
- The initial R wave is a little large than usually seen in LBB but may reflect poor lead placement
- Given the principally negative voltage of the QRS more ST elevation rather than a neutral / subtle depressed ST segment is expected
- There isn’t enough ST elevation to make this lead Sgarbossa positive but I’d be closely looking at serial ECGs for change
What happened next ?
The patient then underwent CABG for treatment of his multi-vessel disease.
- Distal LMCA: 60-70% stenosis
- Proximal LAD: 60-70% stenosis
- Ostial 1st diagonal: 70% stenosis
- Proximal Cx: 80% stenosis
- Mid-RCA: 90% stenosis
The patient then underwent CABG for treatment of his multi-vessel disease.
Sgarbossa Criteria
Smith’s Modified Sgarbossa Criteria AEM Paper
SIMILAR CASE: ECG Case 255