ECG Interpretation
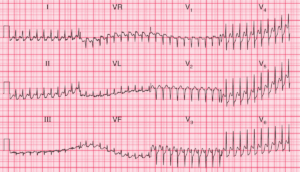
- Regular narrow complex tachycardia, rate about 200/min
- No P waves visible, with possible Pseudo R’ waves in V1 (retrogradely conducted P waves after QRS complex)
- Normal axis
- Regular QRS complexes
- Normal QRS complexes, ST segments and T waves

Clinical Interpretation
This is a supraventricular tachycardia, and since no P waves are visible this is a junctional, or atrioventricular nodal re-entry, tachycardia (AVNRT).
What to do ?
AVNRT is the commonest form of paroxysmal tachycardia in young people, and presumably explains her previous episodes of palpitations.
Attacks of AVNRT may be terminated by any of the manoeuvres that lead to vagal stimulation – Valsalva’s manoeuvre, carotid sinus pressure, or immersion of the face in cold water.
If these are unsuccessful, intravenous adenosine should be given by bolus injection. Adenosine has a very short half-life, but can cause flushing and occasionally an asthmatic attack. If adenosine proves unsuccessful, verapamil 5–10 mg given by bolus injection will usually restore sinus rhythm. Otherwise, DC cardioversion is indicated.