The ECG shows a regular rhythm at a rate of 126 bpm, and the QRS complex duration is increased (0.18 sec). The QRS complex morphology is abnormal (and does not resemble a typical right or left bundle branch block) and the axis is rightward, between +90° and +180° ( negative QRS complex in lead I and positive QRS complex in lead aVF).
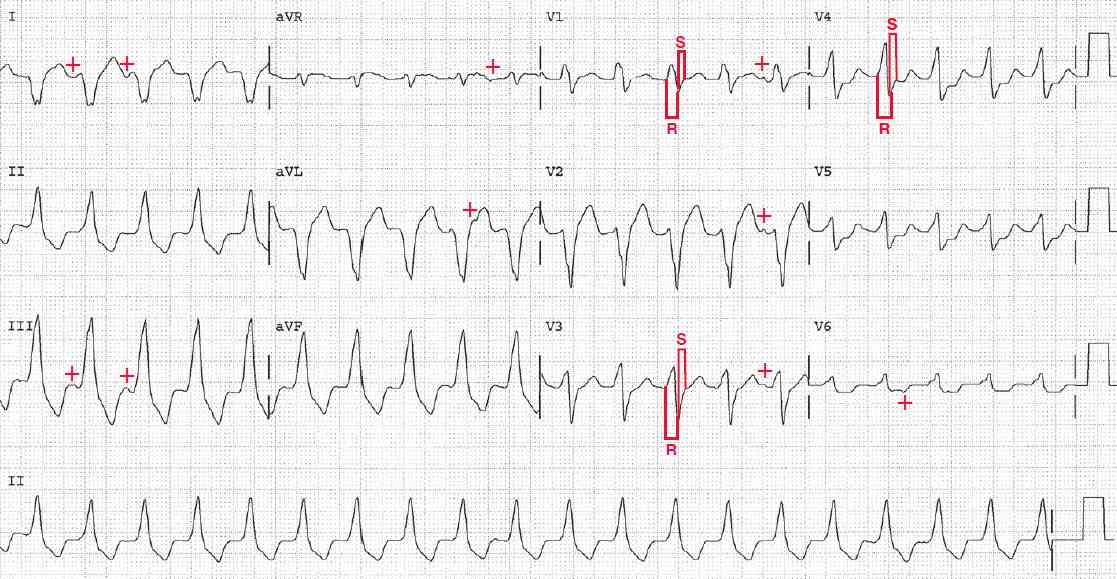
There are no obvious P waves before or after any of the QRS complexes. However, with careful inspection there are subtle changes in the ST segments (+), which is suggestive of atrial activity or P waves. This is seen particularly in leads I and III just prior to the third QRS complex, just after the fourth QRS complex in lead aVL, and just prior to the fifth QRS complex in leads V1-V3.
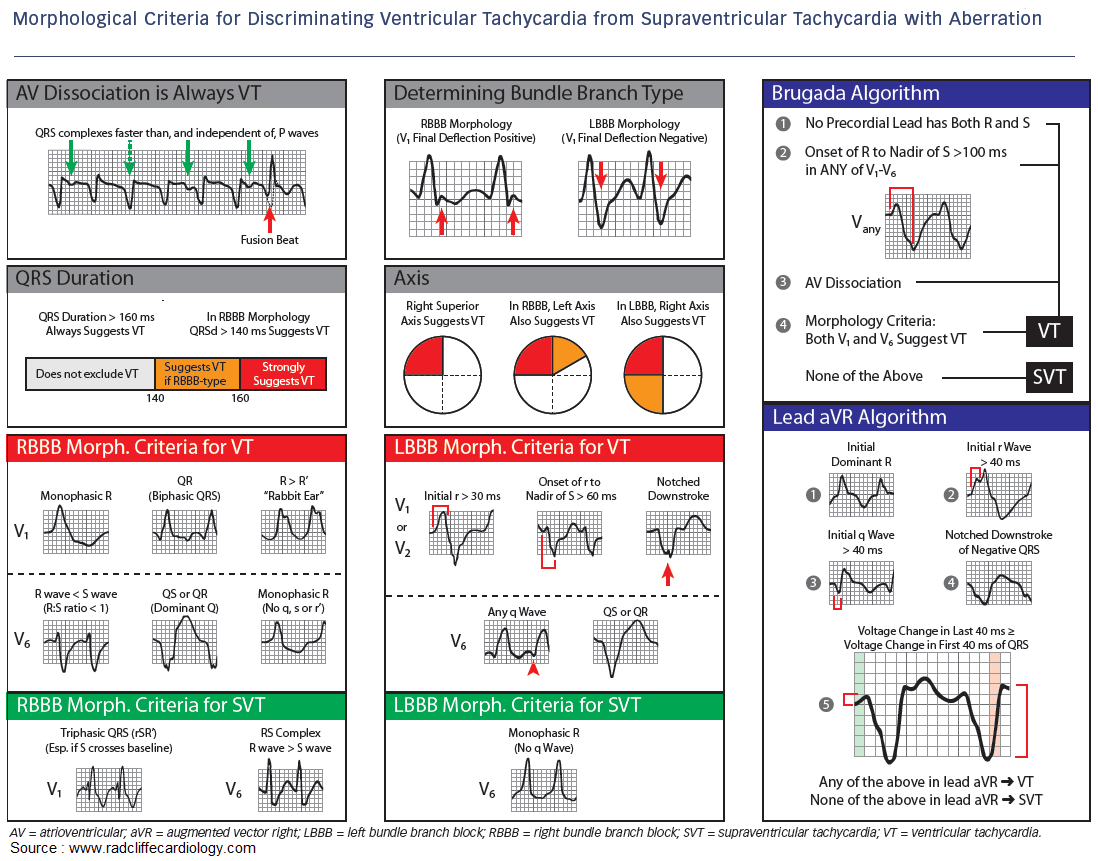
As P waves are seen before some, but not all, of the QRS complexes, this represents AV dissociation. In association with a wide complex tachycardia with an abnormal QRS complex morphology, AV dissociation is characteristic of ventricular tachycardia. As all the QRS complexes have the same morphology, this is monomorphic ventricular tachycardia.
Although the irregularities of the ST segments may not clearly be P waves, such irregularities are seen in ventricular tachycardia and are not seen in supraventricular tachycardia in which there is uniformity of the ST segments as well as QRS complex morphology. This is because activation of the ventricles is via the normal Purkinje system (or an accessory pathway) and the activation sequence (depolarization and repolarization) is the same for each complex.
In addition to AV dissociation, the width of the QRS complex (> 160 msec) is consistent with a diagnosis of ventricular tachycardia.
Also noted is the fact that in leads V1, V3, and V4, which have an RS morphology, the R-wave amplitude is greater than the S-wave depth (ie, R/ S > 1) and the R-wave duration or interval is longer than 100 msec, which means that the initial depolarization of the ventricle is slow and abnormal. This is a feature of a ventricular complex.
Wide QRS complexes due to aberration have an S wave that is wider than the R wave is tall (R/ S < 1) and an R-wave interval or duration that is less than 100 msec because aberration is generally a delay in the terminal forces of the QRS complex. This is one of the Brugada criteria for distinguishing ventricular tachycardia from supraventricular tachycardia with aberration.