The rhythm is regularly irregular with an average rate of 36 bpm. Noted is sagging ST-segment depression (^) with a J point that is at baseline (↑). These ST-segment changes (sagging, hammock-like, or scooping) are typical of digoxin and represent a digoxin effect.
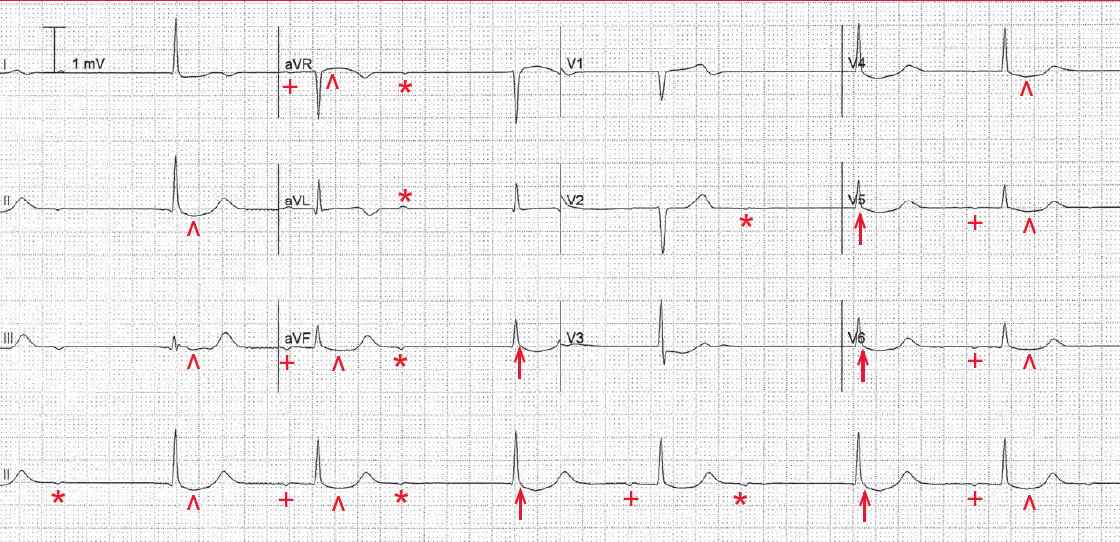
There is evidence of regular atrial activity, at a rate of 58 bpm. The P waves (+) are negative in leads II, aVF, and V5–V6. Hence this is an atrial rhythm.
The second, fourth, and sixth complexes are associated with a stable PR interval (0.26 sec). Following the second and fourth QRS complexes, there is an on-time but nonconducted P wave (*), ie, there is no QRS complex associated with them. Therefore, this is a second-degree AV block.
Following the nonconducted P wave, there is a QRS complex (↑) that does not have a P wave before it and occurs after a pause of 1.8 sec. This QRS complex has the same morphology as the conducted QRS complexes. This is a junctional escape complex that occurs before the next on-time P wave would occur. Hence this is 2:1 AV block with a junctional escape.
The 2:1 AV block is a Mobitz type I, related to a conduction abnormality in the AV node. This AV block is likely the result of the increased vagal effect from digoxin.
Along with the ST segment abnormalities, this ECG represents digoxin excess and probably digoxin toxicity (ie, an atrial tachycardia with second-degree AV block, ie, Mobitz type I).
- READ MORE about Cardiac Glycosides
- SIMILAR CASES: