
This article is an answer to the ECG Case 164
The ECG shows a regular rhythm at a rate of 130 bpm. The QRS complex duration is prolonged (0.22 sec) and the morphology is abnormal, resembling neither a typical right nor left bundle branch block. In addition, there is an indeterminate axis between +/–180° and –90° (QRS complex negative in lead I and aVF).
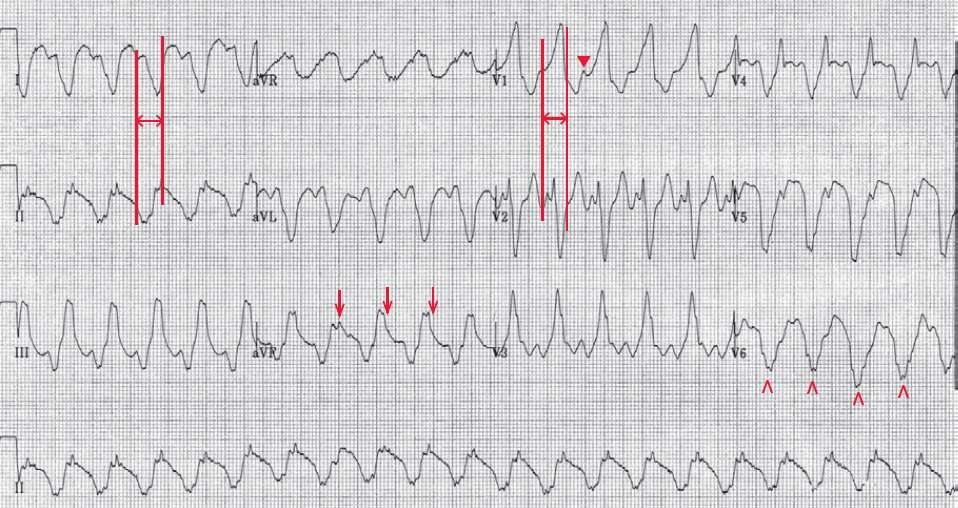
There are no constant P waves seen before or after the QRS complexes. It should be noted that the waveform before the QRS complex in leads I and V2 is part of the QRS complex and not a P wave. This is established by measuring the maximum QRS width as in lead V1 (↔) and comparing the duration to that seen in leads I and V2 (║).
There are occasional P waves seen, for example before the third complex in lead V1 (▼). The presence of a P wave in front of some, but not every, QRS complex is diagnostic for AV dissociation.
There are also subtle differences in QRS morphology (for example in lead V6) (^) and ST-T waves (for example, lead aVF [↓]). Hence this rhythm has a number of findings that are characteristic of ventricular tachycardia (ie, indeterminate axis, evidence of AV dissociation, changes in ST-T waves and QRS complex morphology).
The width of the QRS complex (0.22 sec), which is wider than is usually seen in ventricular tachycardia, suggests that there is an underlying severe cardiomyopathy accounting for a significant degree of intraventricular conduction delay. It is also possible that hyperkalemia is present.
![Read more about the article Hypokalemia ECG Changes [With Examples]](https://manualofmedicine.com/wp-content/uploads/2021/04/Hyperkalemia-and-Hypokalemia-ECG-Changes-2-300x127.jpg)