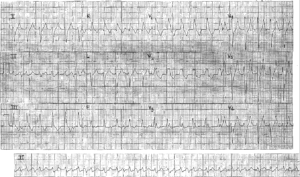
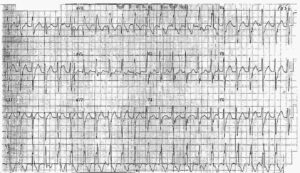
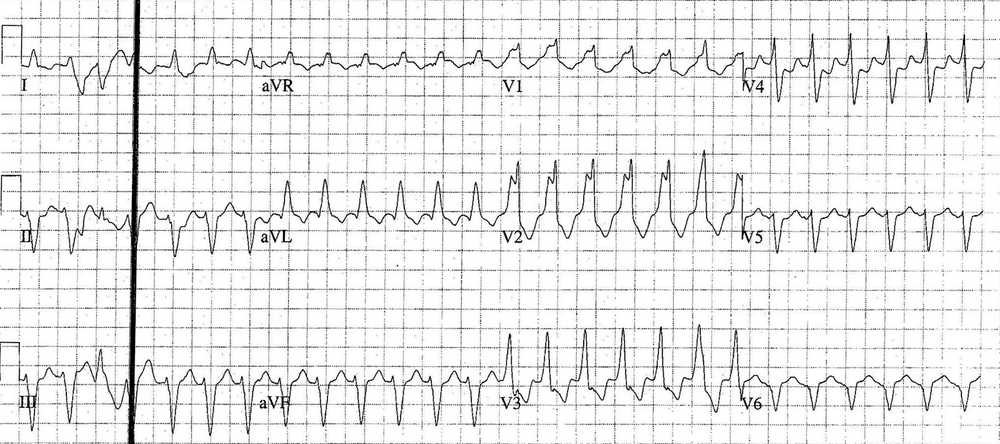
This post is an interpretation of the ECG Case 193
- Rate: ~155 / min
- Rhythm:
- Regular
- Flutter waves ? – best seen in precordial leads esp. V3 with rate ~300bpm
- Axis:
- LAD (-66 deg)
- Intervals:
- QRS – Prolonged (160-200ms)
- QT – 360ms (QTc Bazette ~ 270 ms)
- Segments:
- ST Depression in V2-4, II
- T Inversion in V1-3, I, aVL, aVR
- Additional:
- RBBB Morphology with discordant ST changes
- 3rd & 19th Complexes morphologically different – Fusion ?
- Nil Concordance
Interpretation
- Broad Complex Tachycardia
- Differentials:
- Ventricular Tachycardia
- SVT with aberrant conduction (pre-existing or rate related)
- SVT in setting of pre-excitation
- Right Bundle Branch Block Morphology
- Left Axis Deviation
Our diagnosis is:
- Atrial Flutter 2:1 Block with either pre-existing RBBB or rate-related RBBB
- Bifasicular block
What happened next ?
- Old notes revealed history of Paroxysmal Atrial Fibrillation and a pre-existing RBBB (same morphology as this ECG)
- Patient reviewed by cardiology
- Initially treatment with adensosine with no response
- Underwent DC cardioversion
- Resultant rate – controlled Atrial Fibrillation
- Therapy with oral amiodarone.
- ECHOCARDIOGRAPHY:
- Dilated LV
- Extensive akinese of infero-posterior and lateral walls
- Severe MR
- Mild Pulmonary Hypertension
- Hypokinetic Right Ventricle
- Mod – Severe systolic impairment.
READ MORE:
![Read more about the article Hypokalemia ECG Changes [With Examples]](https://manualofmedicine.com/wp-content/uploads/2021/04/Hyperkalemia-and-Hypokalemia-ECG-Changes-2-300x127.jpg)