This post is an answer to the ECG Case 194
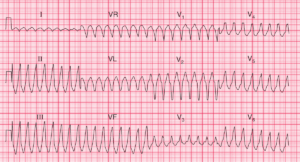
- Rate: ~175 / min
- Rhythm:
- Regular
- No p waves visible
- Axis:
- Extreme Axis Deviation
- Intervals:
- PR – No P waves visible
- QRS – Prolonged (160-200ms)
- Additional:
- Pacing Spikes Visible Intermittently
- Pacing Spikes Interval 1000ms (60 bpm)
- No evidence of pacing capture or fusion
- Spikes best seen Leads II, aVR, V5/6
- No concordance
Interpretation
- Broad Complex Tachycardia
- Consistent with Ventricular Tachycardia
- Patient Age
- Extreme Axis Deviation
- Broad – broad QRS
- Not typical BBB morphology
- Pacing Spikes – Pacer set to VVIR according to old notes
- ? Failure to sense and capture
This patient had a pacemaker inserted 7 years prior to this presentation.
Pacemaker settings:
- Single lead placed in right ventricle
- Pacing mode set to VVIR
- Rate setting 60 – 110 bpm
Why it isn’t Pacemaker Mediated Tachycardia (PMT)
- It can not be a paced rhythm or PMT because of the RBBB morphology unless there is a lead in the left ventricle.
- You need a dual chamber device programmed to at least DDD.
- Results from retrograde conduction of a V paced event sensed as an A and thus tracked over and over.
- The rate of PMT is at or below the upper tracking rate which is not the case here.
The presence of ‘Pacing Spikes’
- Artefactual – Mostly likely by consensus
- The device is at End of Life and is defaulted to VOO mode at 60 bpm – Possibility
- The device battery is low and there is a magnet over it thus making it VOO. The magnet rate is usually 85 or 100 bpm unless the battery is low – Possibility
- The device is at ERI (elective replacement, low battery and thus switched to VVI) and is pacing VVI with loss of sensing – Unlikely
READ MORE: