This post is an answer to the ECG Case 196
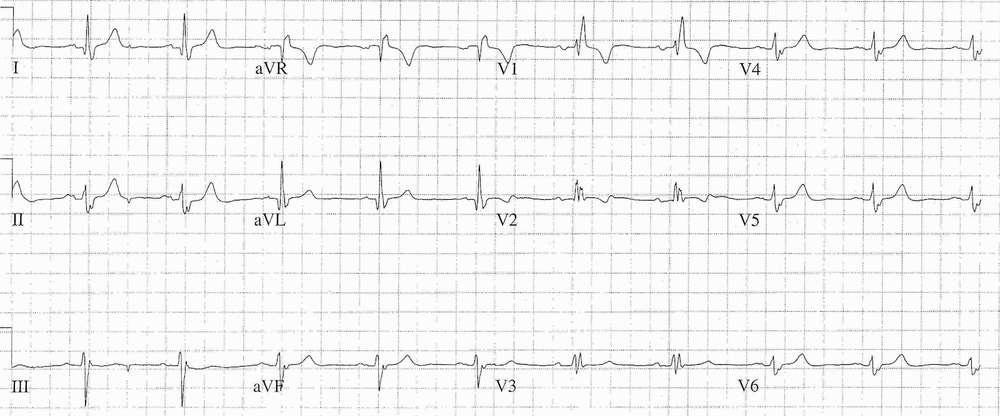
- Rate: ~60 / min
- Rhythm:
- Regular
- Sinus Rhythm
- Axis:
- LAD (<-30 deg)
- Intervals:
- PR – Normal (~180-200ms)
- QRS – Prolonged (140ms)
- QT – 440ms (QTc Bazette ~ 430 ms)
- Additional:
- rsR’ Pattern in V1
- T Inversion in aVR, V1
- Biphasic T wave in V2
- Broad Notched P wave in Lead II
- Notching of baseline following first QRS complex in leads I, II, III – likely artefact
Interpretation
- Bifascicular Block – RBBB + LAFB
- P Mitrale
In the setting of syncope with bifascicular block with features suggestive of cardiac syncope or absence of other clear cause for syncope cardiology referral for consideration of prophylactic pacing is appropriate.(ACC/AHA/HRS 2008 Guidelines Class IIa Level B Recommendation)
The clinical context of a RBBB is important in the clinical decision making. New onset RBBB with symptoms to suggest infarction would make you think of a proximal LAD lesion, proximal to the first septal perforator branch. Note that an LAD occlusion does not give a LBBB.
READ MORE about Pearls in Syncope ECG Interpretation
SIMILAR CASES: