This post is an answer to the ECG Case 208
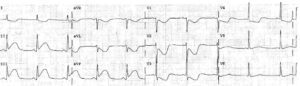
- Rate: ~60 bpm
- Rhythm:
- Regular
- Abnormal p wave axis
- Axis
- LAD (-55 deg)
- Intervals:
- PR – Normal (~12-140ms)
- QRS – Normal (100ms)
- QT – 400ms (QTc Bazette ~ 400 ms)
- Segments:
- ST elevation lead V1 (1mm)
- Up-sloping ST segment lead V2
- Additional:
- T wave inversion in leads II, III, aVF
- P wave inverted in leads II, III, aVF, V1-2
- Notched P wave lead V3
- Positive P wave aVR
- Inferior leads show inversion of not only P wave but also QRS complex and T wave
Interpretation
This ECG is suspicious for limb lead misplacement. On review of the patient the limb electrodes had been misplaced with RA-RL and LA-LL reversal.
This reversal pattern is described as having a flat lead I which is not seen in this ECG. This is likely due to this ECG being recorded using a modified Mason-Likar system; the limb electrodes being placed on the shoulders and abdominal wall, rather than on the ankles and wrists.
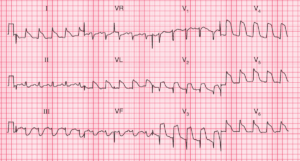
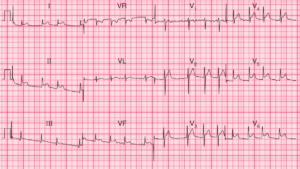
The leads were reapplied in the correct configuration and the ECG was repeated which looked liked this:

Note the resolution of the inferior T wave abnormalities with a normal p wave axis. The P wave in leads V1 and V2 have also changed, this may be due to replacement of the precordial electrodes when the lead misplacement was corrected or due to change in pt position. There is concavity of the inferior ST segments with ST elevation in V1, now <1mm.
READ MORE: ECG Interpretation: All you need to know