
This post is an answer to the ECG Case 233
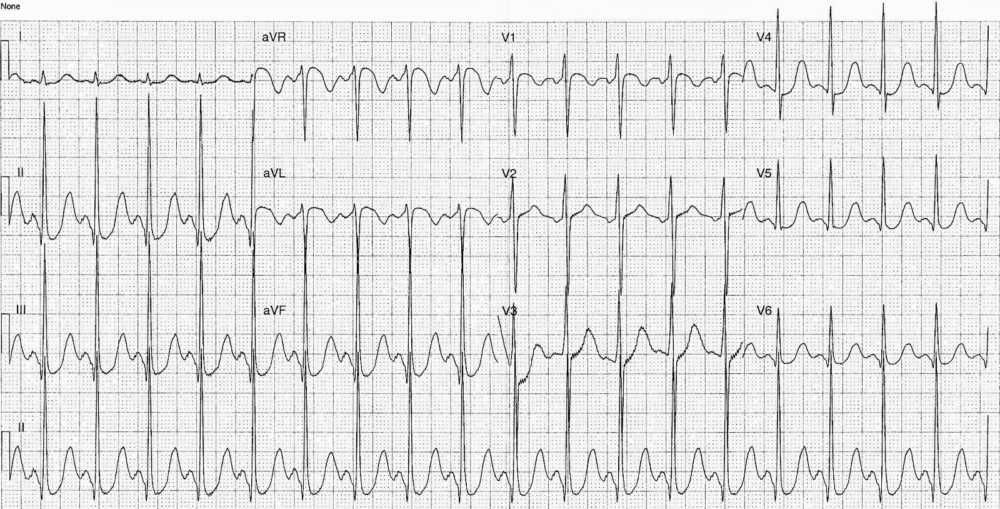
- Rate: ~110 bpm
- Rhythm:
- Regular
- Sinus rhythm
- Axis: Normal
- Intervals:
- PR – Normal (~120ms)
- QRS – Normal (100ms)
- QT – 440ms (QTc Bazette 550-600 ms)
- Segments:
- ST Elevation in leads aVR, aVL and V1
- ST Depression in leads II, III, aVF, V4-6
Interpretation
QTc Prolongation and ST segment changes in this case caused by significant acid-base disturbance (severe alkalaemia).
What happened next?
The patient’s additional biochemistry revealed a primary hypochloraemic metabolic alkalaemia with significant acute renal failure due to recurrent vomiting.
He received titrated benzodiazepines for agitation and following careful re-hydration and electrolyte monitoring the patient’s ECGs normalised. Subsequent upper GI endoscopy revealed an inflammatory gastric outlet obstruction as the cause of his recurrent vomiting.
READ MORE: ECG Interpretation – All you need to know
![Read more about the article Left Ventricular Hypertrophy (LVH): How to Recognize it on ECG [With Examples]](https://manualofmedicine.com/wp-content/uploads/2025/12/Summary-of-the-various-diagnostic-ECG-criteria-for-left-ventricular-hypertrophy-LVH.png)