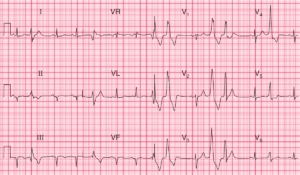
ECG Interpretation
- Sinus rhythm, rate 65/min
- PR interval markedly prolonged (480 ms) – First Degree AV Block
- Normal axis
- Normal QRS complexes
- Deep T wave inversion in leads V1,V2 and biphasic up-down T wave in lead V3

Clinical Interpretation
The deeply inverted T waves in leads V1, V2 and the biphasic (up-down) T wave in lead V3 represent Wellens Syndrome (Critical stenosis of the left anterior descending artery (LAD)).
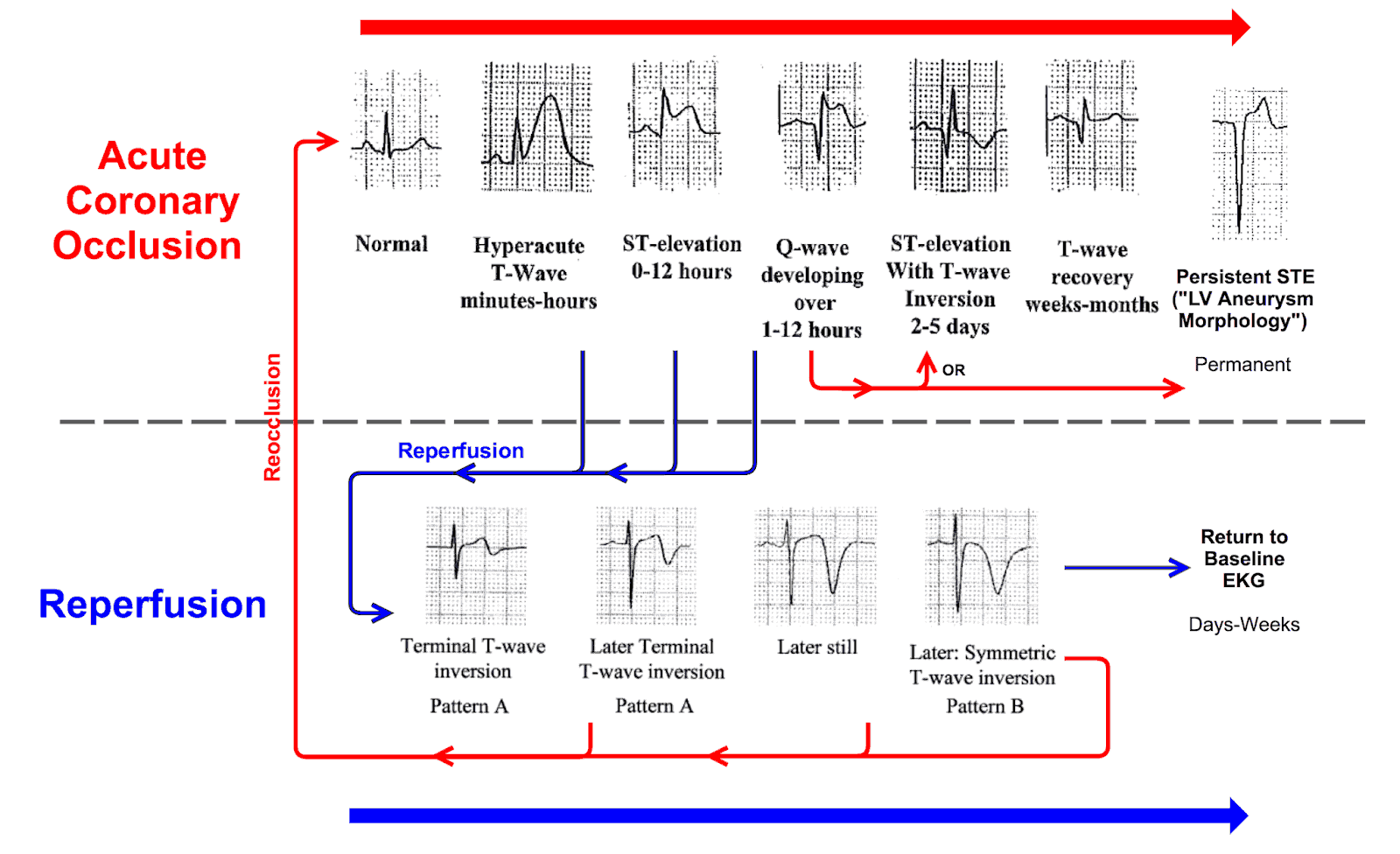
At some time the LAD had been occluded but spontaneous reperfusion has happened (due to spontaneous clot lysis or prehospital aspirin) that resulted in T wave inversion in leads V1-V3 (Wellens Syndrome).
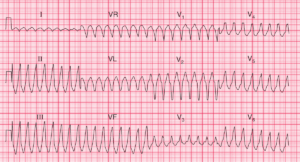
The coronary perfusion is unstable, however, and the LAD can re-occlude at any time.
Since the T wave inversion is in leads V1–V3 but not V4, the possibility of a pulmonary embolus must be considered.
What to do next ?
The ECG changes do not meet the conventional criteria for percutaneous coronary intervention (PCI) or thrombolysis for myocardial infarction (raised ST segments or new left bundle branch block), but the patient does need the full range of treatment for MI – heparin, aspirin, clopidogrel, a beta-blocker, possibly a nitrate, and a statin.
Early angiography must be considered. First degree block is not an indication for temporary pacing, but the patient must be monitored in case higher degrees of block develop.