This post is an answer to the ECG Case 252
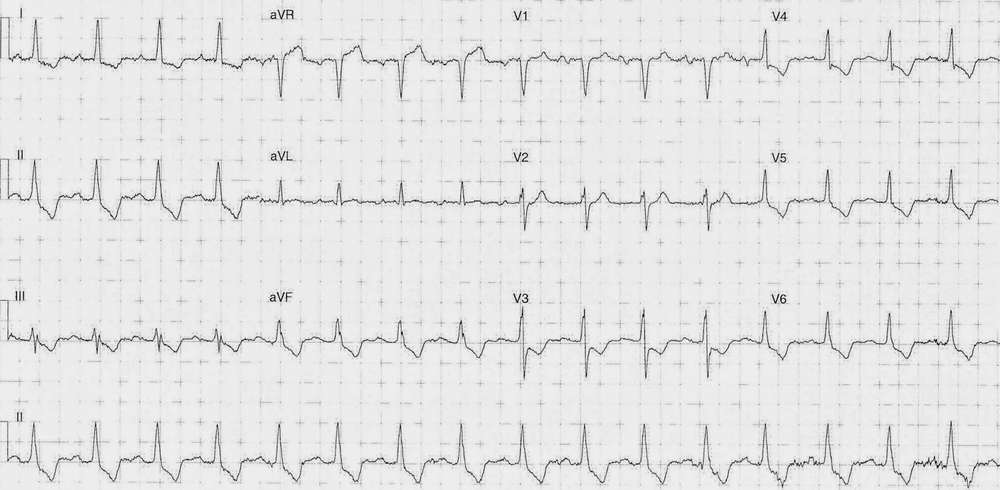
- Rate: 96 bpm
- Rhythm: Regular Sinus rhythm
- Axis: Normal
- Intervals:
- PR – Prolonged (~220ms)
- QRS – Normal (100ms)
- QT – 280ms (QTc Bazette 380 ms)
- Segments:
- ST Elevation in lead aVR (~1.5mm)
- ST Depression in leads I, II, aVF, V3-6
- Additional:
- T wave inversion in leads I, II, III, aVF, V3-6
- Flat T wave in lead aVL
Interpretation
Diffuse ST segment depression with elevation in aVR in the setting of chest pain. Not a traditional STEMI but should prompt major concern for severe left main, LAD stenosis. However, it is not specific for this and can also be sub-endocardial demand ischemia or severe triple vessel disease.
In this patient with a known intra-abdominal perforation the differentials include both sub-endocardial demand ischemia from concurrent illness, but given the history of known coronary artery disease (CAD) could also indicate active ACS.
What happened next?
On discussion with the patient it became apparent she’s been having unstable angina symptoms for several weeks. A prior angiogram from 18 months previous showed a left main severe distal stenosis (90%) with patent stents and vein grafts.
We got an urgent surgical and cardiological opinion as the combination of ACS and intra-abdominal perforation posed a significant management challenge.
The patient received urgent broad-spectrum antibiotic cover and was commenced on heparin with single anti-platelet therapy due to the potential need for surgical intervention. Unfortunately the patient failed conservative treatment with worsening abdominal pain and underwent a laparotomy / washout / resection but suffered a post-procedural cardiac arrest.
SIMILAR CASES: