This post is an answer to the ECG Case 260
Features similar on both ECG’s
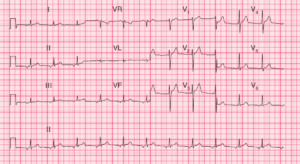
- Rate:
- ECG 1 42 bpm
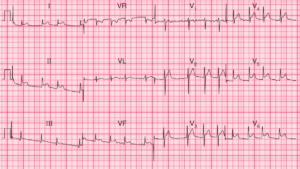
- ECG 2 60 bpm
- Rhythm:
- Sinus Rhythm
- Sinus Arrhythmia
- Axis: Normal
- Intervals:
- PR – Normal (~180ms)
- QRS – Normal (100ms)
Key differences between ECG’s
Segments:
- ECG 1: Flat ST segment elevation in leads V2 and V3
- ECG 1: ST Depression in leads II, III
- ECG 2: Flattening of J point in leads V2 and V3
- ECG 2: Positive T wave in lead V1 with ST elevation in V1

Interpretation
- Dynamic ST segment changes
- Differential Diagnosis:
- ACS in the setting of physiological stress
- Kounis Syndrome
What is Kounis Syndrome ?
First described in 1991 by Dr N Kounis, Kounis syndrome is characterized by a group of symptoms that manifest as unstable vasospastic or non-vasospastic angina secondary to a hypersensitivity reaction and was initially termed ‘allergic angina’.
There are three types of Kounis syndrome:
- Type I: Chest pain secondary to coronary artery vasospasm in patients with no previous history of coronary artery disease
- Type II: Patients with culprit but quiescent pre-existing atheromatous disease in whom the acute release of inflammatory mediators can induce either coronary artery spasm with normal cardiac enzymes and troponins or plaque erosion or rupture manifesting as acute myocardial infarction
- Type III: Patients with coronary thrombosis (including stent thrombosis) in whom aspirated thrombus demonstrate the presence of eosinophils and mast cells respectively