This post is an answer to the ECG Case 265
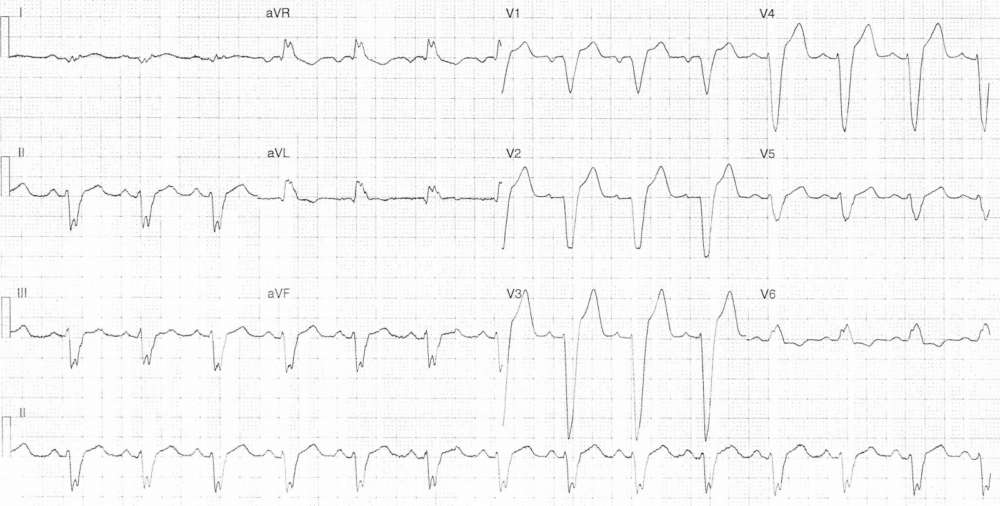
- Rate: 84 bpm
- Rhythm: Regular Sinus Rhythm
- Axis: LAD
- Intervals:
- PR – Normal (~200ms)
- QRS – Prolonged (200ms)
- QT – 400ms
- Segments:
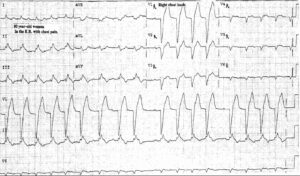
- ST Elevation in leads II, III, aVF, V1-5
- ST Depression in leads aVR, aVL, V6
- ST changes are discordant i.e. in the opposite direction to the QRS vector
- Discordant changes are ‘appropriate’ in magnitude
- Additional:
- T inversion in leads aVR, aVL, V6
- Again discordant to QRS vector
- Deep S wave V1-4
- Notching R wave in V6
- T inversion in leads aVR, aVL, V6
Interpretation
- LBBB
- Sgarbossa / Modified Sgarbossa Negative
- Duration of LBBB unknown – no prior ECG’s available
What happened next?
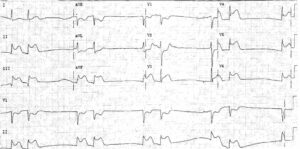
The patient was referred to the cardiology team given his typical history and risk factors. He underwent early coronary angiogram which revealed multi-vessel diffuse disease (<50% stenosis).
An echo showed:
- Mod to severe dilated left ventricle with severe global impairment – EF ~21%
- Mild diastolic dysfunction
- Elevated pulmonary artery pressure with normal right ventricular size & function
The patient was given lifestyle education and commenced on ACE-inhibitor, statin, diuretics and beta-blocker.
‘New’ LBBB remains in the Australian Heart Association guidelines as a trigger for reperfusion therapy. However, the last update of these guidelines was in Sept 2011 and since we have seen a move away from ‘new’ LBBB or ‘presumed new’ LBBB being a trigger for urgent reperfusion.
The American Heart Association 2013 guidelines removed LBBB as an indication for urgent reperfusion. There is clear variation in international guidelines on this topic and clinicians need to be aware of their own local policies and practices regarding reperfusion criteria.
READ MORE: ECG Interpretation – All you need to know