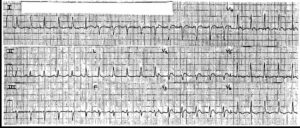
The rhythm is regularly irregular as a result of premature complexes. There are two narrow QRS complexes (^) (duration 0.08 sec), each of which is preceded by a P wave (+) with a stable PR interval (0.16 sec). The P waves are positive in leads I, II, aVF, and V4-V6. Hence, these are sinus complexes.
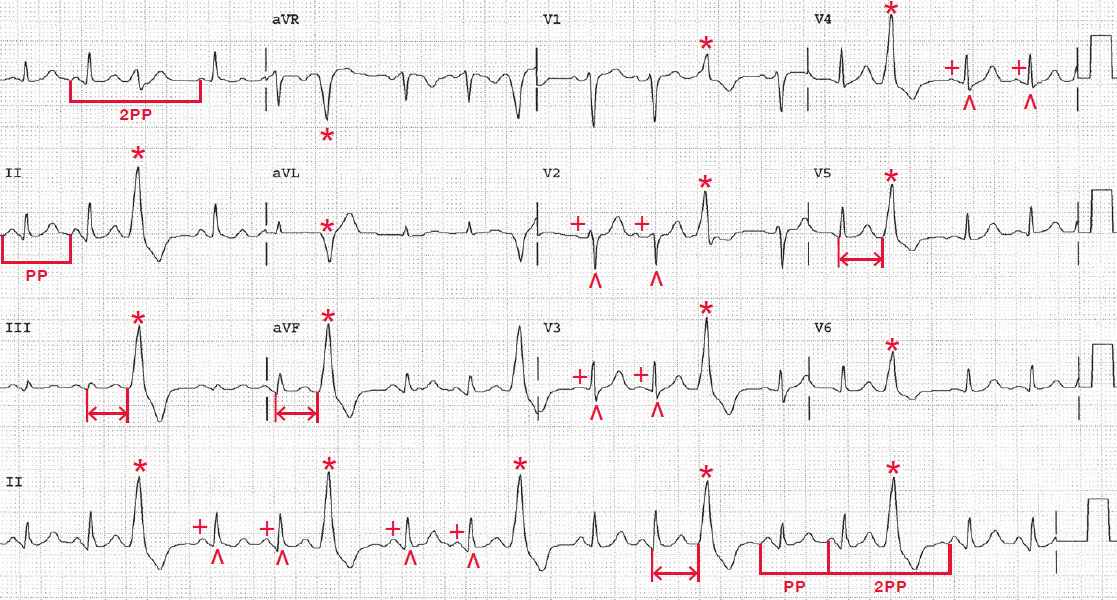
The PP interval is stable, and the rate is 100 bpm. After the two sinus complexes is a premature complex (*) that is wide (duration 0.18 sec) and has an abnormal morphology. Although there is a tall R wave in lead V1, the morphology is not typical for a right bundle branch block as there are no terminal S waves in leads V5-V6.
More importantly, there is positive concordance (ie, tall R waves in leads V1-V6). Positive concordance does not occur as a result of conduction through the normal His-Purkinje system but rather represents direct myocardial activation as occurs with a ventricular complex due to Wolff-Parkinson-White or a paced complex. The QRS complex is not preceded by a P wave. These are premature ventricular complexes (PVCs).
The coupling interval (↔) between the second narrow complex and the PVC is fixed, indicating that the PVC is the result of reentry. Because the PVCs are single, the impulse travels around the circuit only once. Every third QRS complex is a PVC, so this is termed ventricular trigeminy.
Each of the PVCs has the same morphology (ie, they are unifocal). The PVC is followed by a compensatory pause; that is, the PP interval around the PVC is equal to two sinus (PP) intervals (└┘). This is due to the fact that premature impulse enters the AV node retrogradely, causing it to be refractory and unable to conduct the next on-time sinus P wave. The next sinus P wave is conducted normally.
READ MORE: ECG Interpretation – All you need to know