This post is an answer to the Case – Woman With a History of Omental Carcinomatosis
Findings
- Frontal radiograph (Fig. 1) shows increased distance between the stomach bubble and the left aerated lower lung. The right diaphragmatic peak is displaced lateral to the midclavicular line.
- On the lateral projection (Fig. 1), the posterior sulci are blunted, in keeping with pleural effusions.
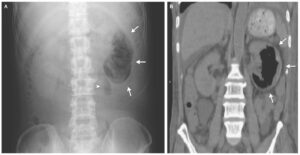
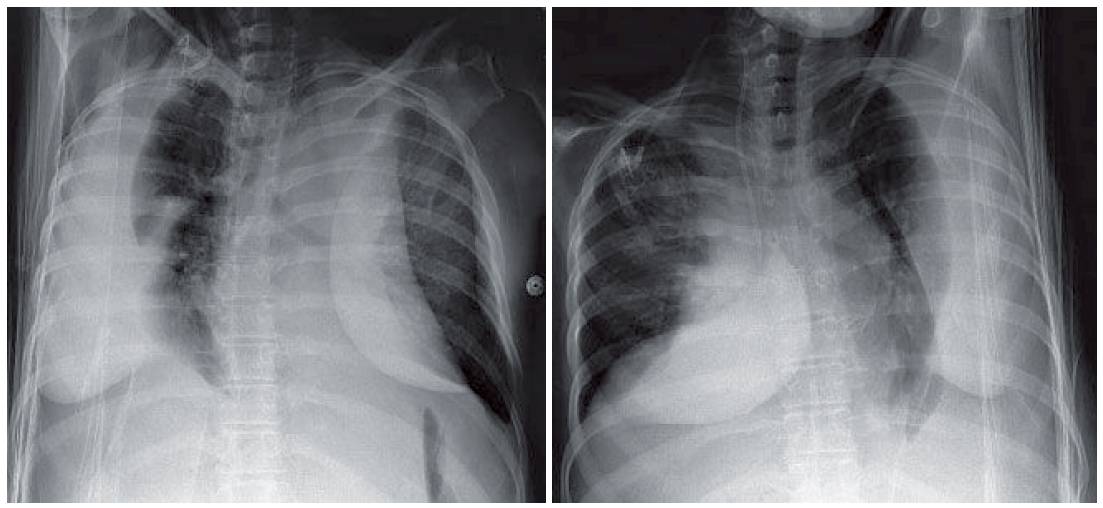
- The large sizes of the pleural effusions are better appreciated on the bilateral decubitus films (Fig. 2).
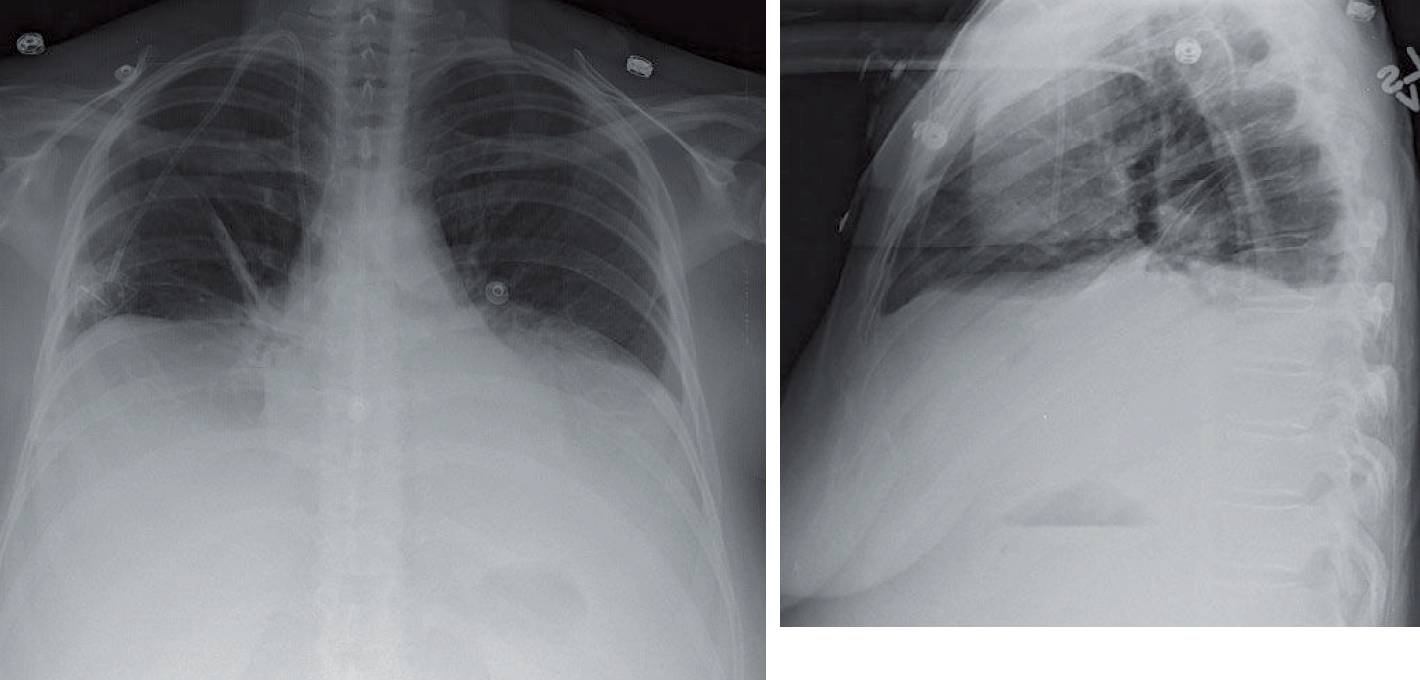
On the lateral projection, the posterior sulci are blunted, in keeping with pleural effusions.
Differential Diagnosis
Bilateral large subpulmonic effusions and small lung volumes with elevated hemidiaphragms are the two main concerns.
Teaching Points
- When pleural fluid collects between the diaphragm and the lower lobe, it is referred to as a subpulmonic effusion.
- A subpulmonic effusion can be very hard to appreciate on an upright frontal radiograph. Findings of a subpulmonic effusion include increased distance between the stomach bubble and the left lung base (over 2 cm) and lateral displacement of the diaphragmatic peak on either side.
- Another sign of a subpulmonic effusion is the lack of visualization of pulmonary vessels below the dome of the diaphragm on the frontal radiograph.
- On the lateral radiograph, some degree of blunting of the posterior sulci is seen. Other findings include a horizontal contour to the diaphragm and fluid partially tracking up the oblique or major fissure (the thorn sign).
- Decubitus films can be performed to confirm the suspicion of the pleural effusion with the fluid layering on the dependent side. The lung parenchyma on the contralateral side can be simultaneously evaluated for an underlying pneumonia. (In this case no underlying pneumonia was seen.)
- At least 175 mL of fluid are required to cause blunting of the costophrenic angles on an upright film. T e lateral decubitus is far more sensitive, detecting as little as 10 mL of fluid if done properly.
Management
- The management of a pleural effusion depends on the nature of the effusion and the clinical symptoms.
- An effusion under tension may require emergent drainage similar to a tension pneumothorax.
- An infected pleural effusion (an empyema) and hemothorax require drainage to prevent the development of a fibrothorax and trapped lung.
References
Yataco JC, Dweik RA. Pleural effusions: evaluation and management. Cleve Clin J Med. 2005 Oct; 72(10): 854-864.