This article is an answer to the Case – Patient with Decreased Level of Consciousness
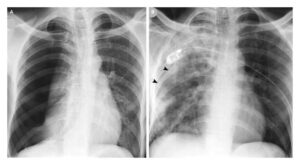
A chest radiograph was obtained at the time of admission showing bilateral upper zonal opacification, with no obvious Kerley B lines or pleural effusions.
A follow-up chest radiograph obtained 2 days later showed rapid resolution of the previously seen upper zonal opacities (image below).

After stabilization from the neurological point of view, the patient was discharged home. The clinical and radiological findings in this case were consistent with neurogenic pulmonary oedema (NPE).
What is neurogenic pulmonary oedema (NPE) ?
NPE is an interesting and under-recognised condition. It is seen in association with acute brain insults, such as intra-cranial haemorrhage, encephalitis or seizures (1, 2).
The patho-physiology is not clearly known, but the process is initiated by increased intra-cranial pressure. This is thought to lead to catecholamine release and a resulting ‘sympathetic storm’, which leads to pulmonary vasoconstriction (hydrostatic mechanism) and leaky capillaries from stress failure (non-cardiogenic mechanism) (2).
The major presentation in cases of NPE is related to the main intra-cranial event, but respiratory symptoms might contribute to the overall picture and necessitate mechanical intubation (1, 2). Given the commonly associated decreased level of consciousness, NPE might be confused for aspiration pneumonitis.
In the context of traumatic related head injuries, it can be confused with pulmonary contusions. Since cases of NPE might be associated with a mild degree of leukocytosis, NPE can be also mistaken for pneumonia. The major hint to the diagnosis is that NPE develops shortly after the intra-cranial insult and resolves quickly within 1-2 days (2).
Although NPE can present with variable appearances on chest radiographs, unilateral or asymmetric bilateral upper zonal lung involvement is a known classic presentation. In contrast to the garden variety cardiogenic pulmonary oedema, features such as Kerely B lines and pleural effusions are usually absent.
Other diagnostic possibilities which might present with bilateral upper zonal pulmonary oedema include: negative pressure pulmonary oedema, high-altitude pulmonary oedema, smoke inhalation and acute mitral regurgitation (2, 3).The respiratory management of NPE is supportive. The main aim of treatment is to control the primary intra-cranial insult (1-3).
References
- Rogers FB, Shackford SR, Trevisani GT, et al. (1995) Neurogenic pulmonary edema in fatal and nonfatal head injuries. J Trauma 39:860-6 (PMID: 7474001)
- Fontes RB, Aguiar PH, Zanetti MV, et al. (2003) Acute neurogenic pulmonary edema: case reports and literature review. J Neurosurg Anesthesiol 15:144-50 (PMID: 12658001)
- Sinoj K. John, and Benjamin D. Morley. (2010) Upper Lobe Predominant Neurogenic Pulmonary Edema In Subarachnoid Hemorrhage. Am J Respir Crit Care Med 181: A6075