This article is an answer to the Case – 71-year-old Woman With Chronic Renal Failure
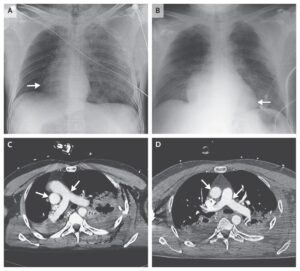
Chest radiograph, HRCT of the chest and a whole-body 99mTc-MDP-scan were performed. Chest radiograph showed diffuse cloudy opacifications in the right upper lobe. On the left side, there was an elevation of the diaphragm, and some pleural effusion.
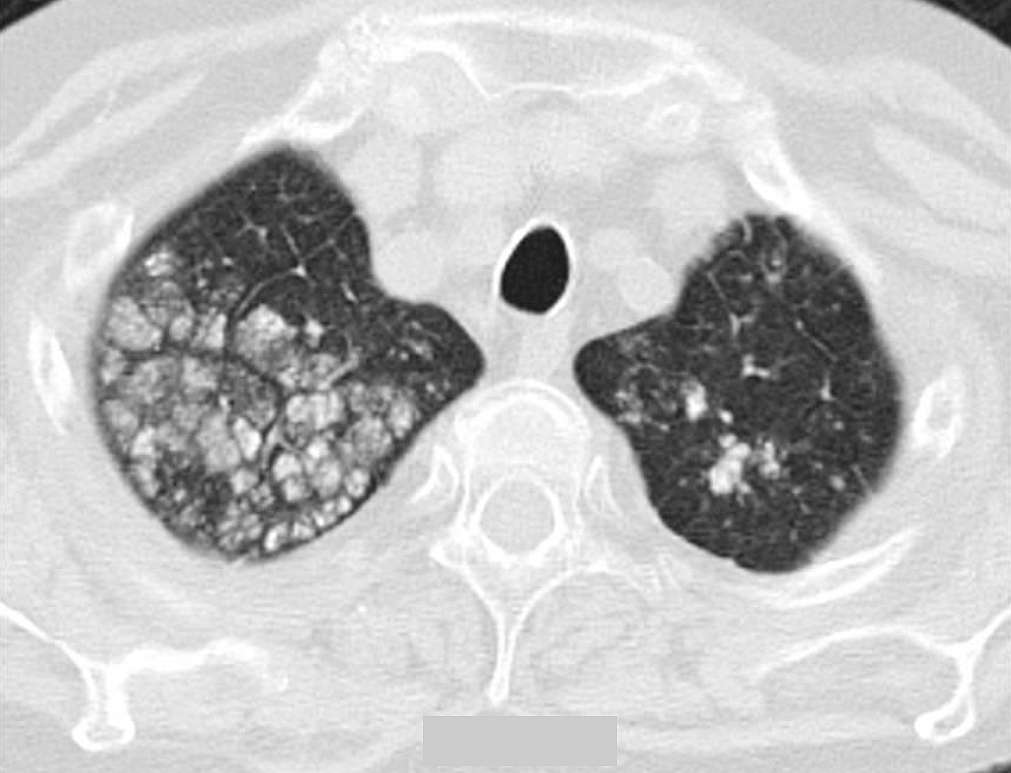
A HRCT of the chest showed multiple nodular, centrilobular and calcified opacities in the right upper lobe, but also, in lesser degree in the left upper lobe, right lower lobe and lingula (see image below). Some of the nodular opacities seen in the right upper lobe demonstrated also punctate calcifications.
A whole-body 99mTc-MDP-scan showed a diffusely increased tracer-uptake at the level of the right upper lobe.
Pulmonary Parenchymal Calcifications
Pulmonary parenchymal calcifications can be divided into dystrophic and metastatic calcifications. Dystrophic lung calcifications are calcifications seen in inflammatory processes, hemorrhage or infarction. Metastatic calcifications occur in diseases with calcium-phosphate disturbance.
The common causes are primary or secondary hyperparathyroidism, chronic renal failure and neoplastic destructive bone lesions as multiple myeloma. In 60 to 75% of patients treated with haemodialysis, metastatic calcifications can be found at autopsy. In extensive pulmonary calcification, a restrictive lung function, a decreased diffusion capacity and hypoxemia can be detected.
In chronic renal failure, four conditions predispose to metastatic calcification:
- Acidosis leaches calcium and phosphate from the bone.
- Kidneys fail to produce vitamin D, which leads to a decrease of calcium uptake. Parathyroid hormone uptake will increase, resulting in an increased calcium and phosphate release from the bone.
- Intermittent alkalosis, which often accompanies haemodialysis, facilitates the precipitation of calcium salts.
- A decreased glomerular filtration of phosphate may contribute to an elevated serum calcium-phosphate product.
Calcium deposition can be found in all parenchymal organs including the lungs. The extent of the physiologic impact associated with calcium deposition does not necessarily correlate with the degree of macroscopic calcification: massive calcifications can be completely asymptomatic.
To detect metastatic pulmonary calcification, chest radiograph is not very effective. HRCT of the chest and 99mTechnetium-methylene diphosphate (99mTc-MDP) bone scintigraphy are more sensitive and specific for the detection of pulmonary calcification.
On HRCT of the chest three patterns of pulmonary parenchymal calcification can be seen:
- Multiple, diffusely or patchy distributed, macroscopically or microscopically calcified nodules
- Diffusely or patchy distributed areas of ground-glass attenuation and
- Dense area(s) of consolidation
The relative stability of these pulmonary infiltrates – in contrast to infectious processes – is of diagnostic value. 99mTc-MDP bone scintigraphy demonstrates calcium deposition, also in lung tissue, and can help in the differential diagnosis of pulmonary lesions.
In patients undergoing haemodialysis or patients with an elevated calcium-phosphate product, metastatic pulmonary calcifications must be taken up in the differential diagnosis of persistent pulmonary parenchymal opacifications. Specific treatment is directed to a correction of isolated hyperphosphatemia or elevated calcium-phosphate product, if present.
References
- Bendayan D, Barziv Y, Kramer MR (2000) Pulmonary calcifications: a review. Respir Med 94:190-193 (PMID: 10783928)
- Yasuo M, Tanabe T, Komatsu Y, Tsushima K, Kubo K, Takahashi K, Kawakami S, Honda T (2008) Progressive Pulmonary Calcification after Successful Renal Transplantation. Intern Med 47:161-164 (PMID: 18239325)
- Chan ED, Morales DV, Welsh CH, McDermott MT, Schwarz MI (2002) Calcium deposition with or without bone formation in the lung. Am J Respir Crit Care Med 165:1654-1669 (PMID: 12070068)
- Braun J (2005) Extraosseous calcification in patients with chronic renal failure-no escape?. Nephrol Dial Transplant 20:2054-2059 (PMID: 16077145)
- Lingam RK, Teh J, Sharma A, Friedman E. (2002) Metastatic pulmonary calcification in renal failure: a new HRCT pattern. Br J Radiol 75:74-77 (PMID: 11806963)